Having enumerated all the possible explanations for my sleepiness and bloating I decided to test out the possibility that it was due to my coming off steroids. I put myself back on 4mg of dexamethasone. My tiredness has left me and the bloating has been much better. In fact I have probably overeaten today since my son and his family was with us and we ate at a restaurant.
Now I must find a way of living with the bigger dose of steroids.
Sunday, July 31, 2011
John 6:14-15. A wrong idea of the Christ
After the people saw the sign Jesus performed, they began to say, “Surely this is the Prophet who is to come into the world.” Jesus, knowing that they intended to come and make him king by force, withdrew again to a mountain by himself.
The Jews of that time had a conception of the Messiah in the image of King David, someone who would overthrow the occupying power and become King of the Jews. Jesus realized how this was likely to play. This is the significance of the 5000 men. He withdrew himself. Did he have an invisibility cloak?
We know that this idea was flawed. Scripture emphasizes that the Christ must suffer fro the sins of the world ut this was too harda concept for them.
The Jews of that time had a conception of the Messiah in the image of King David, someone who would overthrow the occupying power and become King of the Jews. Jesus realized how this was likely to play. This is the significance of the 5000 men. He withdrew himself. Did he have an invisibility cloak?
We know that this idea was flawed. Scripture emphasizes that the Christ must suffer fro the sins of the world ut this was too harda concept for them.
Proteosome inhibitors and HDAC inhibitors
Proteasome inhibitors
Bortezomib modulates protein expression post-translationally by blocking the degradation of a subset of proteins by the proteasome. Although this agent has proved effective in myeloma treatment and CLL cells are sensitive to bortezomib in vitro, poor anti-tumour responses are observed in CLL. Apoptosis induction may be dependent on the post-translational upregulation of the pro-apoptotic NOXA or BAX proteins.
Histone deacetylase inhibitors
Inhibitors of histone deacetylases (HDACs) are a novel class of candidate anti-tumor agent that induce apoptosis by reprogramming patterns of gene expression via modification of the acetylation state of histones. HDAC inhibitor treatment of CLL cells results in upregulation of the pro-apoptotic NOXA and BIM proteins and in apoptosis. NOXA neutralized the antiapoptotic function of the MCL-1 protein and downregulation of MCL-1 expression by CDK inhibitors, including roscovitine-potentiated apoptosis induction by HDAC inhibitors. However, these agents are likely to have a very broad spectrum of targets, which may limit their clinical utility.
Responses were disappointing in phase I trials of the hydroxamate HDAC inhibitor belinostat (no partial or complete remissions) and depsipeptide (no responses by NCI criteria despite substantially increased histone acetylation) and in a phase II trial of the orally available Class I HDAC inhibitor MGCD0103 (no responses). The dose of HDAC inhibitors is likely to be limited by constitutional symptoms including fatigue and nausea. Improved scheduling or combination of HDAC inhibitors with other agents could improve the clinical efficacy of these inhibitors.
Bortezomib modulates protein expression post-translationally by blocking the degradation of a subset of proteins by the proteasome. Although this agent has proved effective in myeloma treatment and CLL cells are sensitive to bortezomib in vitro, poor anti-tumour responses are observed in CLL. Apoptosis induction may be dependent on the post-translational upregulation of the pro-apoptotic NOXA or BAX proteins.
Histone deacetylase inhibitors
Inhibitors of histone deacetylases (HDACs) are a novel class of candidate anti-tumor agent that induce apoptosis by reprogramming patterns of gene expression via modification of the acetylation state of histones. HDAC inhibitor treatment of CLL cells results in upregulation of the pro-apoptotic NOXA and BIM proteins and in apoptosis. NOXA neutralized the antiapoptotic function of the MCL-1 protein and downregulation of MCL-1 expression by CDK inhibitors, including roscovitine-potentiated apoptosis induction by HDAC inhibitors. However, these agents are likely to have a very broad spectrum of targets, which may limit their clinical utility.
Responses were disappointing in phase I trials of the hydroxamate HDAC inhibitor belinostat (no partial or complete remissions) and depsipeptide (no responses by NCI criteria despite substantially increased histone acetylation) and in a phase II trial of the orally available Class I HDAC inhibitor MGCD0103 (no responses). The dose of HDAC inhibitors is likely to be limited by constitutional symptoms including fatigue and nausea. Improved scheduling or combination of HDAC inhibitors with other agents could improve the clinical efficacy of these inhibitors.
Saturday, July 30, 2011
cdk inhibitors
Cyclin-dependent kinase inhibitors
Flavopiridol, roscovitine (CYC202, seliciclib) and SNS-032 are selective inhibitors of cyclin-dependent kinases (Cdks) 7 and 9. These Cdks phosphorylate critical serine residues in the carboxy-terminal domain of RNA polymerase II, thereby enabling this enzyme to initiate and elongate RNA transcripts. The rationale for these agents in cancer treatment is that short-lived anti-apoptotic proteins are depleted more rapidly in response to transcription inhibition than long-lived proteins following Cdk inhibition. Flavopiridol, roscovitine and SNS-032 inhibit C-terminal phosphorylation of RNA polymerase II, decrease cellular levels of the anti-apoptotic proteins Mcl-1 and XIAP and induce apoptosis of CLL cells in vitro.
Flavopiridol killed CLL cells in vitro regardless of previous treatment history. Killing was independent of the expression of anti-apoptotic Bcl-2 relative to pro-apoptotic Bax, whereas the toxicity of fludarabine was strongly dependent on this ratio. Flavopiridol induced partial remissions (40%) with a median progression-free survival duration of 12 months, even in patients refractory to fludarabine or with poor-risk genetic features (i.e. deletion of TP53 or ATM genes). A Phase II trial confirmed the conclusions of the Phase I study and indicated that the dosing schedule was critical. Prophylactic dexamethasone might improve tolerability by reducing the risk of the cytokine release syndrome.
Roscovitine induced apoptosis of CLL cells and downregulation of pro-survival proteins including Mcl-1, probably by inhibition of RNA polymerase phosphorylation and is in clinical trials for solid tumours.
Limited clinical activity of SNS-032 was seen in a Phase I clinical trial of SNS-032, with tumour lysis syndrome as the dose-limiting toxicity. Further modification of drug doses and scheduling are likely to be required to maximize the clinical efficacy of this agent and of other CDK inhibitors.
Flavopiridol, roscovitine (CYC202, seliciclib) and SNS-032 are selective inhibitors of cyclin-dependent kinases (Cdks) 7 and 9. These Cdks phosphorylate critical serine residues in the carboxy-terminal domain of RNA polymerase II, thereby enabling this enzyme to initiate and elongate RNA transcripts. The rationale for these agents in cancer treatment is that short-lived anti-apoptotic proteins are depleted more rapidly in response to transcription inhibition than long-lived proteins following Cdk inhibition. Flavopiridol, roscovitine and SNS-032 inhibit C-terminal phosphorylation of RNA polymerase II, decrease cellular levels of the anti-apoptotic proteins Mcl-1 and XIAP and induce apoptosis of CLL cells in vitro.
Flavopiridol killed CLL cells in vitro regardless of previous treatment history. Killing was independent of the expression of anti-apoptotic Bcl-2 relative to pro-apoptotic Bax, whereas the toxicity of fludarabine was strongly dependent on this ratio. Flavopiridol induced partial remissions (40%) with a median progression-free survival duration of 12 months, even in patients refractory to fludarabine or with poor-risk genetic features (i.e. deletion of TP53 or ATM genes). A Phase II trial confirmed the conclusions of the Phase I study and indicated that the dosing schedule was critical. Prophylactic dexamethasone might improve tolerability by reducing the risk of the cytokine release syndrome.
Roscovitine induced apoptosis of CLL cells and downregulation of pro-survival proteins including Mcl-1, probably by inhibition of RNA polymerase phosphorylation and is in clinical trials for solid tumours.
Limited clinical activity of SNS-032 was seen in a Phase I clinical trial of SNS-032, with tumour lysis syndrome as the dose-limiting toxicity. Further modification of drug doses and scheduling are likely to be required to maximize the clinical efficacy of this agent and of other CDK inhibitors.
John 6: 10-13. Jesus Creator
Jesus said, “Have the people sit down.” There was plenty of grass in that place, and they sat down (about five thousand men were there). Jesus then took the loaves, gave thanks, and distributed to those who were seated as much as they wanted. He did the same with the fish. When they had all had enough to eat, he said to his disciples, “Gather the pieces that are left over. Let nothing be wasted.” So they gathered them and filled twelve baskets with the pieces of the five barley loaves left over by those who had eaten.
This miracle is reminiscent of Elijah and the widow at Zarephath whose jug of flour and jar of oil was never used up and Elisha and the widow's cruze of oil. We are also told that this was a sign. What does the sign describe? It reminds us that Jesus is the Creator of the universe, who can make barley loaves and little fish with impunity.
Recycling began here; waste not want not.
This miracle is reminiscent of Elijah and the widow at Zarephath whose jug of flour and jar of oil was never used up and Elisha and the widow's cruze of oil. We are also told that this was a sign. What does the sign describe? It reminds us that Jesus is the Creator of the universe, who can make barley loaves and little fish with impunity.
Recycling began here; waste not want not.
When to use capitals
If you have been reading the signaling papers (and I know that they are not everybody's cup of tea) you ought to be aware of the molecular biologists convention for the names of genes and proteins.
Genes are generally cited in italics - so we have SYK or BCR-ABL - whereas the proteins produced from them are given in capitals: SYK or BCR-ABL or BCL2.
However, if we are talking about mouse proteins rather than human proteins the names are given in lower case letters: bcl2 and lyn and bid.
I am not a molecular biologist, so I do make mistakes here.
Genes are generally cited in italics - so we have SYK or BCR-ABL - whereas the proteins produced from them are given in capitals: SYK or BCR-ABL or BCL2.
However, if we are talking about mouse proteins rather than human proteins the names are given in lower case letters: bcl2 and lyn and bid.
I am not a molecular biologist, so I do make mistakes here.
Thalidomide made respectable by NICE; what next?
One of the headlines this week was that NICE has approved thalidomide for the treatment of myeloma. Since thalidomide was such a bete noir of the investigative press all those years ago, it was worth a mention on the BBC News. Today there is a good article on thalidomide and its derivatives, lenalidomide and pomalidomide (collectively known as IMiDs), in Cancer Treatment Reviews from the German group that includes Stephan Stilgenbauer and Harmut Dohner, of whom I am such a big fan. The three diseases that they are valuable in, Myeloma, MDS and CLL, are the three diseases that I have spent most of my life studying.
The anti-inflammatory role of thalidomide was discovered by chance after giving it as sedative to a leprosy patient suffering from erythema nodosum leprosum. The underlying molecular mechanism was later shown to involve inhibition of the B-cell receptor, which is necessary for antigen-induced activation of the immune system.
In contrast, Rho GTPase-dependent intracellular signaling seems to be activated by pomalidomide, a third-generation IMiD, resulting in reorganization of the cytoskeleton and enhanced cellular migration.
In multiple myeloma there seems to be a direct cytotoxic effect of immune modulatory drugs on tumor cells that are resistant to conventional therapy. It is mediated via inhibition of NFκB and induction of caspase 8 activity. In contrast, in CLL cells an induction of NFκB and NFAT-signaling has been reported for lenalidomide together with activation of PI3K-activity, resulting in enhanced transcription and mRNA stabilization of the CD154 receptor that itself also mediates activation of the canonical and non-canonical NFκB signaling pathway. Completely opposite effects in CLL and myeloma! In CLL, the induction of NFκB leads to increased expression of pro-apoptotic molecules like BID and DR5 which sensitize CLL cells to TRAIL-induced apoptosis, but also seems to reverse the humoral tolerance against tumor specific antigens like ROR1, suggesting a dual mode of action.
In the minimally deleted region on chromosome 5q in MDS, two phosphatases (CDC25C and PP2A) have been identified that control the transition of G2 to M in the cell cycle. These dual-specificity serine threonine phosphatases are deleted in the majority of del 5q MDS patients and are also inhibited in their enzymatic activity by lenalidomide. The subsequent inhibition of cell proliferation could be the reason why del 5q MDS patients are especially sensitive to treatment with the drug. The expression of the tumor suppressor gene SPARC that is also localized in the critical region on 5q. Incubation of del 5q cells, which have low levels of SPARC, with lenalidomide upregulated the gene back to normal levels. The proposed function of SPARC is as a cell cycle inhibitor and counteradhesive factor.
Another cell cycle inhibitor that is upregulated by lenalidomide in Burkitt-lymphoma and MM-derived cell lines is the CDKN1A/p21/WAF gene. I am afraid that the mechanism for this happening, which involves epigenetics is too complicated to explain to you. I must ask my daughter what it means.
An elevation of TNFa production is implicated in the pathogenesis of a number of hematopoietic malignancies including CLL. TNFa levels are reduced after treatment
with lenalidomide as early as 7 days after the beginning of therapy. This reduction correlates with a decrease in the white blood cell count.
Thalidomide and its derivatives may influence cytokine patterns differently, allowing them to be grouped into two different classes depending on whether they increase levels of IL-2, IL-10, IFN gamma, and the activity of phosphodiesterase 4 and decrease of TNFa, IL-1ß and IL-6. IL-6 is known to inhibit the apoptosis of malignant myeloma cells and help in their proliferation. In-vitro, the production of IL-6 is directly downregulated by lenalidomide, which results in the reduction of osteolysis and changes in the tumor microenvironment. In MM patients however, there is an increase in levels of IL-6 upon treatment with lenalidomide, and IL-6 (together with IL-10, IL-2 and TNFaR1) is also increased on day 7 after treatment with lenalidomide in patients with CLL , suggesting a transient immune activation in these patients.
Changes in cytokine patterns subsequently lead to changes in the composition of
the lymphocyte compartment, which had already been observed in patients suffering from leprosy, where the T-helper cell compartment was increased after treatment with thalidomide. Thalidomide has been shown to act as costimulator to CD3 engagement, activating CD8+ T-cells.
However, the activation of T-cells is dependent on the IMiD used, with one group of second-generation drugs lacking this activating capacity. In-vitro, immune modulatory drugs act on T-cells via the B7-CD28 co-stimulatory pathway. Blockade of this interaction can be overcome by incubation with IMiDs, but not via upregulation of B7 or CD28 on T-cells or antigen presenting cells (APC), rather, they induce phosphorylation of CD28, resulting in activation of downstream targets like PI3K and NFκB and subsequent activation of the T-cell. This T-cell stimulation results in increased secretion of IFN gamma and IL-2, the Th1-type cytokine response, and can stimulate clonal T-cell proliferation and NK cell activity.
In 50% of patients with MDS but only in 5% of age-matched controls, a clonal expansion of effector T-cells with natural killer (NK) surface markers (e.g. NKG2D) is observed by analyzing T-cell receptor clonality at the CDR-3. In patients with MDS, CLL or MM, treatment with lenalidomide results in an antigen-dependent increase in NK cell populations. In addition, in vitro experiments have also shown an increased killing capacity of NK-cells towards MM cells after treatment with IMiDs. Both thalidomide and lenalidomide also seems to enhance the immune response in CLL patients by downregulating the number of suppressive regulatory T-cells (CD4+ CD25high FOXP3+). Similarly, pro-inflammatory IL-17 positive regulatory T-cells are upregulated in CLL patients at a later stage after treatment with lenalidomide.
In CLL the formation of the immunological synapse between the malignant B-cells and the T-cells is impaired, possibly due to aberrant actin polymerization and subsequent
reduction of polarity of the T-cells. This lack of polarization is also induced in T-cells from healthy donors by CLL cells. However, upon treatment with lenalidomide, the in vitro capacity of T-cells to form an immunological synapse can be recovered.
One of the key elements of the pathology of hematological diseases is the interaction of the malignant cells with the bone marrow. The adhesion of tumor cells to bone marrow stromal cells often induces the secretion of pro-angiogenic and other cytokines, which are essential for the pathogenesis of the disease.
Bone marrow stromal cells (BMSC) are required for normal hematopoiesis, but also give pro-survival and proliferative support to MM cells. The close interaction between MM cells and BMSCs is partially based on the induction of secretion of IL-6 and VEGF from BMSCs by VEGF secreted from MM cells. This interaction can be inhibited by neutralizing antibodies directed against IL-6 or VEGF, but inhibition is more practically induced clinically by treatment with thalidomide.
In contrast, in 5q- MDS it seems that IMiDs do not directly impact on the microenvironment, rather that eradication of the MDS clone leads to restoration of normal stromal function.
Malignant cells from the peripheral blood and lymph node aspirates of CLL patients undergo rapid apoptosis when taken out of the patient and cultured in vitro, a process which can be rescued by co-culture with stromal cells in vitro. In addition, a reduction of the immunocompetence of non-malignant cells can be observed upon co-culture with CLL cells. These interdependencies of CLL cells with their stromal microenvironment may be one of the reasons why IMiDs are effective in the treatment of this disease, blocking the pro-survival support and possibly reinstating the suppressed immunocompetence of the CLL microenvironment. It remains to be seen whether the observed tumor flare reactions that occur in the lymph nodes of CLL patients upon treatment with high doses of lenalidomide is due to the re-establishment of the immune competence of the microenvironment in these organs.
In MM, there is increased bone marrow microvascular density and VEGF levels. Both thalidomide and lenalidomide inhibit angiogenesis.
As patients with del5q MDS respond best to lenalidomide compared to patients without the deletion, levels of VEGF and its receptor KDR were analyzed in MDS patients responding to lenalidomide treatment. In line with VEGF signaling being a major target for IMiD function, both VEGF and KDR were found to be significantly
downregulated in MDS patients responding to treatment and this downregulation proved to be a prognostic factor for induction of remission.
Co-culture of CLL cells on stromal cells induces a pro-angiogenic phenotype in CLL cells including enhanced expression of VEGF, a process that is reminiscent of the interaction of MM cells with their BM microenvironment. The exact molecular mechanism remains unclear.
Early trials of third generation IMiDs like pomalidomide are promising. In a phase I clinical trial of pomalidomide treatment in relapsed MM patients, only 3/24 patients developed thrombosis, the treatment-related non-hematologic dose-limiting toxicity. Thalidomide-resistant patients were allowed, but still the ORR was 53% with four CRs.
An even more promising therapeutic strategy is the combination of IMiDs with compounds targeting either different proteins within the same pathways like dexamethasone, or the combination with therapeutics that target different pathways and therefore act synergistically.
The anti-inflammatory role of thalidomide was discovered by chance after giving it as sedative to a leprosy patient suffering from erythema nodosum leprosum. The underlying molecular mechanism was later shown to involve inhibition of the B-cell receptor, which is necessary for antigen-induced activation of the immune system.
In contrast, Rho GTPase-dependent intracellular signaling seems to be activated by pomalidomide, a third-generation IMiD, resulting in reorganization of the cytoskeleton and enhanced cellular migration.
In multiple myeloma there seems to be a direct cytotoxic effect of immune modulatory drugs on tumor cells that are resistant to conventional therapy. It is mediated via inhibition of NFκB and induction of caspase 8 activity. In contrast, in CLL cells an induction of NFκB and NFAT-signaling has been reported for lenalidomide together with activation of PI3K-activity, resulting in enhanced transcription and mRNA stabilization of the CD154 receptor that itself also mediates activation of the canonical and non-canonical NFκB signaling pathway. Completely opposite effects in CLL and myeloma! In CLL, the induction of NFκB leads to increased expression of pro-apoptotic molecules like BID and DR5 which sensitize CLL cells to TRAIL-induced apoptosis, but also seems to reverse the humoral tolerance against tumor specific antigens like ROR1, suggesting a dual mode of action.
In the minimally deleted region on chromosome 5q in MDS, two phosphatases (CDC25C and PP2A) have been identified that control the transition of G2 to M in the cell cycle. These dual-specificity serine threonine phosphatases are deleted in the majority of del 5q MDS patients and are also inhibited in their enzymatic activity by lenalidomide. The subsequent inhibition of cell proliferation could be the reason why del 5q MDS patients are especially sensitive to treatment with the drug. The expression of the tumor suppressor gene SPARC that is also localized in the critical region on 5q. Incubation of del 5q cells, which have low levels of SPARC, with lenalidomide upregulated the gene back to normal levels. The proposed function of SPARC is as a cell cycle inhibitor and counteradhesive factor.
Another cell cycle inhibitor that is upregulated by lenalidomide in Burkitt-lymphoma and MM-derived cell lines is the CDKN1A/p21/WAF gene. I am afraid that the mechanism for this happening, which involves epigenetics is too complicated to explain to you. I must ask my daughter what it means.
An elevation of TNFa production is implicated in the pathogenesis of a number of hematopoietic malignancies including CLL. TNFa levels are reduced after treatment
with lenalidomide as early as 7 days after the beginning of therapy. This reduction correlates with a decrease in the white blood cell count.
Thalidomide and its derivatives may influence cytokine patterns differently, allowing them to be grouped into two different classes depending on whether they increase levels of IL-2, IL-10, IFN gamma, and the activity of phosphodiesterase 4 and decrease of TNFa, IL-1ß and IL-6. IL-6 is known to inhibit the apoptosis of malignant myeloma cells and help in their proliferation. In-vitro, the production of IL-6 is directly downregulated by lenalidomide, which results in the reduction of osteolysis and changes in the tumor microenvironment. In MM patients however, there is an increase in levels of IL-6 upon treatment with lenalidomide, and IL-6 (together with IL-10, IL-2 and TNFaR1) is also increased on day 7 after treatment with lenalidomide in patients with CLL , suggesting a transient immune activation in these patients.
Changes in cytokine patterns subsequently lead to changes in the composition of
the lymphocyte compartment, which had already been observed in patients suffering from leprosy, where the T-helper cell compartment was increased after treatment with thalidomide. Thalidomide has been shown to act as costimulator to CD3 engagement, activating CD8+ T-cells.
However, the activation of T-cells is dependent on the IMiD used, with one group of second-generation drugs lacking this activating capacity. In-vitro, immune modulatory drugs act on T-cells via the B7-CD28 co-stimulatory pathway. Blockade of this interaction can be overcome by incubation with IMiDs, but not via upregulation of B7 or CD28 on T-cells or antigen presenting cells (APC), rather, they induce phosphorylation of CD28, resulting in activation of downstream targets like PI3K and NFκB and subsequent activation of the T-cell. This T-cell stimulation results in increased secretion of IFN gamma and IL-2, the Th1-type cytokine response, and can stimulate clonal T-cell proliferation and NK cell activity.
In 50% of patients with MDS but only in 5% of age-matched controls, a clonal expansion of effector T-cells with natural killer (NK) surface markers (e.g. NKG2D) is observed by analyzing T-cell receptor clonality at the CDR-3. In patients with MDS, CLL or MM, treatment with lenalidomide results in an antigen-dependent increase in NK cell populations. In addition, in vitro experiments have also shown an increased killing capacity of NK-cells towards MM cells after treatment with IMiDs. Both thalidomide and lenalidomide also seems to enhance the immune response in CLL patients by downregulating the number of suppressive regulatory T-cells (CD4+ CD25high FOXP3+). Similarly, pro-inflammatory IL-17 positive regulatory T-cells are upregulated in CLL patients at a later stage after treatment with lenalidomide.
In CLL the formation of the immunological synapse between the malignant B-cells and the T-cells is impaired, possibly due to aberrant actin polymerization and subsequent
reduction of polarity of the T-cells. This lack of polarization is also induced in T-cells from healthy donors by CLL cells. However, upon treatment with lenalidomide, the in vitro capacity of T-cells to form an immunological synapse can be recovered.
One of the key elements of the pathology of hematological diseases is the interaction of the malignant cells with the bone marrow. The adhesion of tumor cells to bone marrow stromal cells often induces the secretion of pro-angiogenic and other cytokines, which are essential for the pathogenesis of the disease.
Bone marrow stromal cells (BMSC) are required for normal hematopoiesis, but also give pro-survival and proliferative support to MM cells. The close interaction between MM cells and BMSCs is partially based on the induction of secretion of IL-6 and VEGF from BMSCs by VEGF secreted from MM cells. This interaction can be inhibited by neutralizing antibodies directed against IL-6 or VEGF, but inhibition is more practically induced clinically by treatment with thalidomide.
In contrast, in 5q- MDS it seems that IMiDs do not directly impact on the microenvironment, rather that eradication of the MDS clone leads to restoration of normal stromal function.
Malignant cells from the peripheral blood and lymph node aspirates of CLL patients undergo rapid apoptosis when taken out of the patient and cultured in vitro, a process which can be rescued by co-culture with stromal cells in vitro. In addition, a reduction of the immunocompetence of non-malignant cells can be observed upon co-culture with CLL cells. These interdependencies of CLL cells with their stromal microenvironment may be one of the reasons why IMiDs are effective in the treatment of this disease, blocking the pro-survival support and possibly reinstating the suppressed immunocompetence of the CLL microenvironment. It remains to be seen whether the observed tumor flare reactions that occur in the lymph nodes of CLL patients upon treatment with high doses of lenalidomide is due to the re-establishment of the immune competence of the microenvironment in these organs.
In MM, there is increased bone marrow microvascular density and VEGF levels. Both thalidomide and lenalidomide inhibit angiogenesis.
As patients with del5q MDS respond best to lenalidomide compared to patients without the deletion, levels of VEGF and its receptor KDR were analyzed in MDS patients responding to lenalidomide treatment. In line with VEGF signaling being a major target for IMiD function, both VEGF and KDR were found to be significantly
downregulated in MDS patients responding to treatment and this downregulation proved to be a prognostic factor for induction of remission.
Co-culture of CLL cells on stromal cells induces a pro-angiogenic phenotype in CLL cells including enhanced expression of VEGF, a process that is reminiscent of the interaction of MM cells with their BM microenvironment. The exact molecular mechanism remains unclear.
Early trials of third generation IMiDs like pomalidomide are promising. In a phase I clinical trial of pomalidomide treatment in relapsed MM patients, only 3/24 patients developed thrombosis, the treatment-related non-hematologic dose-limiting toxicity. Thalidomide-resistant patients were allowed, but still the ORR was 53% with four CRs.
An even more promising therapeutic strategy is the combination of IMiDs with compounds targeting either different proteins within the same pathways like dexamethasone, or the combination with therapeutics that target different pathways and therefore act synergistically.
Friday, July 29, 2011
Aphorisms 16
If you think the world a place intended only for our happiness you will find it quite intolerable – CS Lewis
I didn’t go into religion to make me happy; I always knew a bottle of port would do that. – CS Lewis
It seems to me that the ‘extreme’ elements in every church are the nearest to one another; while the ‘liberal’ and ‘broad-minded’ could never be united at all. – CS Lewis
Most political sermons teach us nothing except which newspapers are read in the Rectory. – CS Lewis
Now that contraceptives have removed the uncharitable element in fornication I do not expect people to recognize it as a sin until they have accepted Christianity as a whole. - CS Lewis
'A good police force is one that catches more crooks than it employs.' – Sir Robert Mark
If we cannot lay down our tastes, along with other carnal baggage, at the church door, surely we should at least bring them in to be humbled and, if necessary, modified, not to be indulged? – CS Lewis
I didn’t go into religion to make me happy; I always knew a bottle of port would do that. – CS Lewis
It seems to me that the ‘extreme’ elements in every church are the nearest to one another; while the ‘liberal’ and ‘broad-minded’ could never be united at all. – CS Lewis
Most political sermons teach us nothing except which newspapers are read in the Rectory. – CS Lewis
Now that contraceptives have removed the uncharitable element in fornication I do not expect people to recognize it as a sin until they have accepted Christianity as a whole. - CS Lewis
'A good police force is one that catches more crooks than it employs.' – Sir Robert Mark
If we cannot lay down our tastes, along with other carnal baggage, at the church door, surely we should at least bring them in to be humbled and, if necessary, modified, not to be indulged? – CS Lewis
John 6: 8-9. One greater than Elisha
Another of his disciples, Andrew, Simon Peter’s brother, spoke up, “Here is a boy with five small barley loaves and two small fish, but how far will they go among so many?”
In the past there has been a tendency to spiritualize the bread and fish so that the two fish are made to represent the two sacraments, Baptism and the Lord's Supper and teh 5 loaves the other five sacraments of the Roman Catholic church, but this is puerile. We are just supposed to see the futility of feeding so many with so little. Again Liberals have suggested that everybody had their packed lunches and the young man volunteering his shamed them into producing theirs. That's just a device to avoid the miraculous.
There is an obscure story in 2 Kings 4:42 about Elisha feeding a hundred men with just 20 loaves (barley loaves as here) and there was food left over. Perhaps that story is hinted at here, but one greater than Elisha is here!
In the past there has been a tendency to spiritualize the bread and fish so that the two fish are made to represent the two sacraments, Baptism and the Lord's Supper and teh 5 loaves the other five sacraments of the Roman Catholic church, but this is puerile. We are just supposed to see the futility of feeding so many with so little. Again Liberals have suggested that everybody had their packed lunches and the young man volunteering his shamed them into producing theirs. That's just a device to avoid the miraculous.
There is an obscure story in 2 Kings 4:42 about Elisha feeding a hundred men with just 20 loaves (barley loaves as here) and there was food left over. Perhaps that story is hinted at here, but one greater than Elisha is here!
More on Heat Shock Proteins
Heat-shock protein (Hsp) inhibitors
Hsps play key roles in maintaining correctly folded conformations of multiple signalling proteins. Hsp90 inhibitors, including the ansamycins, geldanamycin and its derivatives 17-allylamino 17-demethoxygeldanamycin (17-AAG) and 17-dimethylaminoethylamino-17-demethoxygeldanamycin (17-DMAG), all target multiple pathways that selectively maintain the malignant phenotype. This may be because of preferential degradation of mutant oncoproteins following Hsp90 inhibition and the increased dependence of malignant cells on key Hsp90-dependent survival-signalling proteins compared to non-malignant cells.
Ansamycins destabilize signalling proteins critical to CLL cell survival, including Lyn, ZAP-70 and AKT. 17-DMAG destabilizes Ikk in vitro, thus decreasing active NF-κB and transcription of its pro-survival target genes. 17-DMAG also prolonged survival in a TCL1A-severe combined immunodeficiency transplant model of CLL. Interestingly, geldanamycin upregulated pro-apoptotic wild-type TP53 (p53) while destabilizing mutant oncogenic TP53.
Ansamycins kill CLL cells in synergy with chlorambucil, fludarabine or rituximab, preferentially induce CLL apoptosis relative to normal lymphocytes or CD34+ bone marrow progenitors and kill CLL cells regardless of prognostic criteria. In clinical trials in solid tumour patients 17-AAG was well tolerated and showed significant antitumour activity. The favourable indications resulting from in vitro and animal model studies and the ability of ansamycins to target multiple anti-apoptotic proteins in CLL suggest that these agents may be ideal candidates for novel therapeutic approaches.
2-phenylacetylenesulfonamide (PAS) is an inhibitor of the Hsp70 chaperone protein. PAS kills CLL cells at concentrations that are non-toxic to CD34+ stem cells. The CLL cell killing was at least partially dependent on the induction of the Noxa pro-apoptotic protein in response to accumulation of unfolded proteins.
Hsps play key roles in maintaining correctly folded conformations of multiple signalling proteins. Hsp90 inhibitors, including the ansamycins, geldanamycin and its derivatives 17-allylamino 17-demethoxygeldanamycin (17-AAG) and 17-dimethylaminoethylamino-17-demethoxygeldanamycin (17-DMAG), all target multiple pathways that selectively maintain the malignant phenotype. This may be because of preferential degradation of mutant oncoproteins following Hsp90 inhibition and the increased dependence of malignant cells on key Hsp90-dependent survival-signalling proteins compared to non-malignant cells.
Ansamycins destabilize signalling proteins critical to CLL cell survival, including Lyn, ZAP-70 and AKT. 17-DMAG destabilizes Ikk in vitro, thus decreasing active NF-κB and transcription of its pro-survival target genes. 17-DMAG also prolonged survival in a TCL1A-severe combined immunodeficiency transplant model of CLL. Interestingly, geldanamycin upregulated pro-apoptotic wild-type TP53 (p53) while destabilizing mutant oncogenic TP53.
Ansamycins kill CLL cells in synergy with chlorambucil, fludarabine or rituximab, preferentially induce CLL apoptosis relative to normal lymphocytes or CD34+ bone marrow progenitors and kill CLL cells regardless of prognostic criteria. In clinical trials in solid tumour patients 17-AAG was well tolerated and showed significant antitumour activity. The favourable indications resulting from in vitro and animal model studies and the ability of ansamycins to target multiple anti-apoptotic proteins in CLL suggest that these agents may be ideal candidates for novel therapeutic approaches.
2-phenylacetylenesulfonamide (PAS) is an inhibitor of the Hsp70 chaperone protein. PAS kills CLL cells at concentrations that are non-toxic to CD34+ stem cells. The CLL cell killing was at least partially dependent on the induction of the Noxa pro-apoptotic protein in response to accumulation of unfolded proteins.
Thursday, July 28, 2011
Signaling in CLL: Inhibition of translation
The regulation of translational initiation
The Mek/Erk pathway regulates protein translation initiation via activation of the 90 kDa ribosomal S6 kinase p90RSK. The PI-3K/Akt pathway controls translation via a different pathway, involving the activation of a multi-subunit protein kinase complex, mTorc1. Both p90RSK and mTorc1 phosphorylate the ribosomal S6 protein, thereby altering the spectrum of mRNAs translated by the ribosome in a manner that may serve to block apoptosis. P90RSK may also block apoptosis via mechanisms distinct from translation control.
mTorc1 and p90RSK as potential therapeutic targets in CLL
The mTorc1 inhibitor rapamycin and its analogs temsirolimus, everolimus and deferolimus are in clinical trials against solid tumours. While constitutive activation of Akt in CLL remains controversial, mTorc1 can also be activated via the Erk pathway, which is also activated in CLL. Therefore, mTorc1 is a potential therapeutic target in this malignancy.
Rapamycin induces a G1 phase cell cycle arrest in CLL cells stimulated to proliferate by treatment with CpG-containing oligonucleotides and IL-2. The inhibitor also blocks phosphorylation of the mTorc1 target p70S6K. However, rapamycin fails to induce significant apoptosis of either cycling or quiescent cells. Rapamycin toxicity was similar in CLL cells and in normal peripheral blood mononuclear cells. The inhibitor induced synergistic killing when combined with chlorambucil or vincristine, but antagonized killing by fludarabine or cyclophosphamide.
Rapamycin inhibited S6 phosphorylation in vivo in the CLL-like malignant cells of Eμ-TCL1A transgenic mice, but their treatment with the inhibitor did not prolong survival.
Six of eight heavily pre-treated CLL patients achieved stable disease in a phase II single-agent trial of deferolimus. A trial of everolimus (RAD001) induced one partial remission and three cases of stable disease but it was terminated after the enrolment of only seven patients due to toxicity. Only four of 22 patients achieved partial remissions in a phase II study of oral everolimus in refractory CLL, but malignant cells were mobilized from bone marrow and lymph nodes and entered the peripheral circulation, with a consequent reduction of lymphadenopathy. Rapamycin analogs may therefore, have value in removing CLL cells from cytoprotective microenvironments.
In summary, in vitro data as well as clinical experience using rapamycin analogs is disappointing. These agents may be of value when used in carefully formulated combinations with conventional agents. Dual inhibitors targeting mTorc1 and PI-3k may be more effective than mTorc1 inhibitors alone, due to their ability to block the feedback activation of PI-3k resulting from mTor inhibition. The dual inhibitor NVP-BEZ235 strikingly inhibited growth of human lymphoma cells in vitro and in a mouse xenograft model. NVP-BEZ235 is in clinical trials for solid tumours and its actions on CLL cells should be evaluated.
A new generation of inhibitors that, unlike rapamycins, directly target the ATP-binding site of the mTorc1 protein kinase are currently entering clinical trials against solid tumours. These agents include OSI-027 and AZD8055 and Torin 1. Torin 1 was disappointingly only marginally toxic towards CLL cells, even at concentrations that effectively inhibited mTorc1. This may be because of increased autophagy with mTorc1 inhibition. In contrast, BI-D1870, a highly selective inhibitor of p90RSK, is substantially more toxic. Inhibition of the p90RSK arm of the translational control machinery may therefore be a better therapeutic approach in CLL than inhibition of mTorc1.
The Mek/Erk pathway regulates protein translation initiation via activation of the 90 kDa ribosomal S6 kinase p90RSK. The PI-3K/Akt pathway controls translation via a different pathway, involving the activation of a multi-subunit protein kinase complex, mTorc1. Both p90RSK and mTorc1 phosphorylate the ribosomal S6 protein, thereby altering the spectrum of mRNAs translated by the ribosome in a manner that may serve to block apoptosis. P90RSK may also block apoptosis via mechanisms distinct from translation control.
mTorc1 and p90RSK as potential therapeutic targets in CLL
The mTorc1 inhibitor rapamycin and its analogs temsirolimus, everolimus and deferolimus are in clinical trials against solid tumours. While constitutive activation of Akt in CLL remains controversial, mTorc1 can also be activated via the Erk pathway, which is also activated in CLL. Therefore, mTorc1 is a potential therapeutic target in this malignancy.
Rapamycin induces a G1 phase cell cycle arrest in CLL cells stimulated to proliferate by treatment with CpG-containing oligonucleotides and IL-2. The inhibitor also blocks phosphorylation of the mTorc1 target p70S6K. However, rapamycin fails to induce significant apoptosis of either cycling or quiescent cells. Rapamycin toxicity was similar in CLL cells and in normal peripheral blood mononuclear cells. The inhibitor induced synergistic killing when combined with chlorambucil or vincristine, but antagonized killing by fludarabine or cyclophosphamide.
Rapamycin inhibited S6 phosphorylation in vivo in the CLL-like malignant cells of Eμ-TCL1A transgenic mice, but their treatment with the inhibitor did not prolong survival.
Six of eight heavily pre-treated CLL patients achieved stable disease in a phase II single-agent trial of deferolimus. A trial of everolimus (RAD001) induced one partial remission and three cases of stable disease but it was terminated after the enrolment of only seven patients due to toxicity. Only four of 22 patients achieved partial remissions in a phase II study of oral everolimus in refractory CLL, but malignant cells were mobilized from bone marrow and lymph nodes and entered the peripheral circulation, with a consequent reduction of lymphadenopathy. Rapamycin analogs may therefore, have value in removing CLL cells from cytoprotective microenvironments.
In summary, in vitro data as well as clinical experience using rapamycin analogs is disappointing. These agents may be of value when used in carefully formulated combinations with conventional agents. Dual inhibitors targeting mTorc1 and PI-3k may be more effective than mTorc1 inhibitors alone, due to their ability to block the feedback activation of PI-3k resulting from mTor inhibition. The dual inhibitor NVP-BEZ235 strikingly inhibited growth of human lymphoma cells in vitro and in a mouse xenograft model. NVP-BEZ235 is in clinical trials for solid tumours and its actions on CLL cells should be evaluated.
A new generation of inhibitors that, unlike rapamycins, directly target the ATP-binding site of the mTorc1 protein kinase are currently entering clinical trials against solid tumours. These agents include OSI-027 and AZD8055 and Torin 1. Torin 1 was disappointingly only marginally toxic towards CLL cells, even at concentrations that effectively inhibited mTorc1. This may be because of increased autophagy with mTorc1 inhibition. In contrast, BI-D1870, a highly selective inhibitor of p90RSK, is substantially more toxic. Inhibition of the p90RSK arm of the translational control machinery may therefore be a better therapeutic approach in CLL than inhibition of mTorc1.
Explanation versus reasons. Why am I so tired?
Doctors are good at giving explanations. I have been scratching my head over the cause of my symptoms, which are uncomfortable abdominal bloating and extreme tiredness, so that I fall asleep as soon as I sit down.
Here are some explanations:
1 It is all the result of the chemotherapy - someone told me that the side effects persist as long as the course of treatment - in my case 6 months. Someone else said it takes at least a year to get over them.
2 It is still the neuropathy caused by the oxaloplatin
3 It is the surgical effect of the anastamosis. a] it is the blind loop left by the surgery causing i)dumping syndrome; ii) excessive insulin secretion; iii) exaggerated gastro-colic secretion. b] it is sluggish flow because the narrow anastamosis. c] it is caused by bacterial overgrowth. d] it is caused by fungal overgrowth.
4 It is caused by a low potassium because I have been on steroids for so long.
5 It is steroid induced myopathy
6 It is because I am reducing the steroids
7 It is because I am anemic
8 It is all in the mind
9 I am depressed at the prospect of dying
10 I am depressed because I have retired and not found a new role
11 I have aged three years since I've had this disease and what I have are the symptoms of old age.
12 I have been fighting it long enough and I am ready to give up
13 I have a scan coming up and I am anxious
14 The cancer has come back.
You see an explanation is not the same as a reason. Without evidence an explanation is just speculation
Here are some explanations:
1 It is all the result of the chemotherapy - someone told me that the side effects persist as long as the course of treatment - in my case 6 months. Someone else said it takes at least a year to get over them.
2 It is still the neuropathy caused by the oxaloplatin
3 It is the surgical effect of the anastamosis. a] it is the blind loop left by the surgery causing i)dumping syndrome; ii) excessive insulin secretion; iii) exaggerated gastro-colic secretion. b] it is sluggish flow because the narrow anastamosis. c] it is caused by bacterial overgrowth. d] it is caused by fungal overgrowth.
4 It is caused by a low potassium because I have been on steroids for so long.
5 It is steroid induced myopathy
6 It is because I am reducing the steroids
7 It is because I am anemic
8 It is all in the mind
9 I am depressed at the prospect of dying
10 I am depressed because I have retired and not found a new role
11 I have aged three years since I've had this disease and what I have are the symptoms of old age.
12 I have been fighting it long enough and I am ready to give up
13 I have a scan coming up and I am anxious
14 The cancer has come back.
You see an explanation is not the same as a reason. Without evidence an explanation is just speculation
John 6:7. Not a hole in the corner affair.
Philip answered him, “Eight months’ wages would not buy enough bread for each one to have a bite!”
It was actually more than 200 dinarii in the Greek. The dinarius was a day's wage for a working man.
What I want to emphasize is how over the top is the amount. These miracles in John's gospel were not hole in the corner affairs. The water turned into wine in was six 20-30 gallon jars. The woman at the well had had 5 husbands, not just a couple, the man had been waiting for 38 years for the water to stir and now here it would have required more than eight month's wages even to give every one a bite!. Jesus was being extravagant in his miracle working. He will still walk on water and raise the dead.
No wonder there were crowds.
It was actually more than 200 dinarii in the Greek. The dinarius was a day's wage for a working man.
What I want to emphasize is how over the top is the amount. These miracles in John's gospel were not hole in the corner affairs. The water turned into wine in was six 20-30 gallon jars. The woman at the well had had 5 husbands, not just a couple, the man had been waiting for 38 years for the water to stir and now here it would have required more than eight month's wages even to give every one a bite!. Jesus was being extravagant in his miracle working. He will still walk on water and raise the dead.
No wonder there were crowds.
Wednesday, July 27, 2011
Erk signaling

The extracelluar signal-regulated kinase (Erk) pathway
The Ras guanine nucleotide-binding proteins exist in an inactive GDP-bound form in unstimulated cells. Activation of receptor-associated PTKs results in the replacement of GDP by GTP, thus switching the Ras protein to an active conformation. GTP-bound Ras then activates the Raf protein kinase, triggering in turn the mitogen-activated protein kinase (Mek) and Erk. Erk-mediated phosphorylation of transcription factors including serum response factor (SRF) initiates cell-cycle entry via transcriptional upregulation of cell-cycle genes. Erk activation also blocks apoptosis, at least in part by phosphorylation of the pro-apoptotic protein Bim, resulting in Bim degradation within the proteasome.
Constitutive Erk activation in CLL cells
Malignant cells isolated from some CLL patients express constitutively activated Erk. Downregulation of active Erk precedes apoptosis induced by the Syk inhibitor R406. Treatment of CLL cells with flavopiridol or the vitamin D3 analog EB1089 decreases active Erk and induces apoptosis of CLL cells, suggesting that constitutive Erk activity confers apoptosis resistance. In vitro studies which investigate downstream consequences of Mek/Erk inhibition and its impact on apoptosis are needed to determine the role of this pathway in CLL. These studies may enhance attempts to target this pathway in a clinical setting.
John 6:5-6. Jesus knew what he was doing.
When Jesus looked up and saw a great crowd coming toward him, he said to Philip, “Where shall we buy bread for these people to eat?” He asked this only to test him, for he already had in mind what he was going to do.
Philip was a local man so he was an obvious person to ask. Mark tells us that Jesus had spent time teaching the crowd, so they would have been tired and hungry.
Jesus already had in mind what he was going to do.
The feeding of the five thousand men (who knows hoe many women and children has echoes of stories from Elijah and Elisha as well as God's marvelous provision in the desert after the Exodus. We will see Jesus claim to be the bread of life and hear an outrageous claim that sounds like cannibalism. Bread will be equated with flesh and this will point forward to the Eucharist. This story is one of the most vivid in the whole Bible.
Philip was a local man so he was an obvious person to ask. Mark tells us that Jesus had spent time teaching the crowd, so they would have been tired and hungry.
Jesus already had in mind what he was going to do.
The feeding of the five thousand men (who knows hoe many women and children has echoes of stories from Elijah and Elisha as well as God's marvelous provision in the desert after the Exodus. We will see Jesus claim to be the bread of life and hear an outrageous claim that sounds like cannibalism. Bread will be equated with flesh and this will point forward to the Eucharist. This story is one of the most vivid in the whole Bible.
Tuesday, July 26, 2011
NFkappaB in CLL

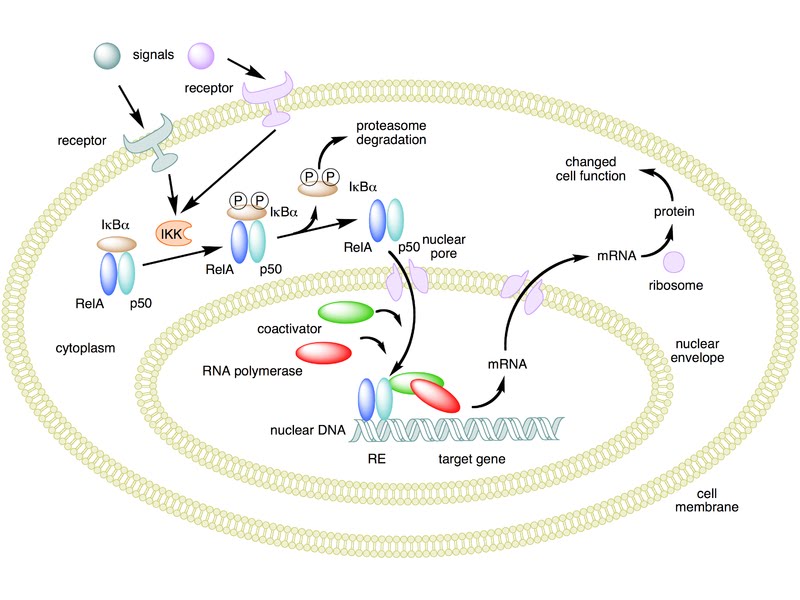
The NF-κB family of transcription factors consists of p50, p52, RelA (also known as p65), c-Rel and RelB subunits. When two of these (the same two or a different two) come together as a dimer it forms an active transcription factor. Anti-apoptotic proteins including Bcl-2 family members Bfl-1 and Bcl-XL, the cellular inhibitors of apoptotic proteases (cIAPs) 1 and 2 and X-linked IAP (XIAP), are potential targets of NF-κB.
In uninduced normal cells, NF-κB dimers are bound by inhibitor of κB (IκB) proteins and sequestered in an inactive form in the cytoplasm. Consequent to BCR signalling, PKCβ activates the IκB kinase (Ikk) complex by the intermediate participation of a complex containing the proteins Carma-1, Malt1 and Bcl10, which activates the Tak1 protein kinase. Activation of Ikk by Tak1 results in IκB phosphorylation, ubiquitination and degradation, leading to activation of NF-κB. The PI-3K/Akt pathway also contributes to NF-κB activation in B cells.A
NF-κB in CLL
Nuclear-localized NF-κB is constitutively elevated in CLL cells compared to normal B and T lymphocytes. NF-κB elevation in peripheral blood CLL cells and consequent upregulation of Bcl-2, Bcl-XL and Mcl-1 may be mediated at least in part by interactions with vascular endothelial cells. DNA-bound (i.e. transcriptionally active) levels of the p65 subunit correlated well with in vitro survival of CLL cells, in vitro fludarabine resistance, Binet stage, time to first treatment and overall survival. No correlations were observed between nuclear p65 levels and IGHV, CD38 or Zap-70 status.
The Ikk inhibitor parthenolide and its derivative LC1 induces apoptosis of CLL cells. Sensitivity of individual isolates to LC1 correlate well with constitutive levels of nuclear-localized p65 subunit. A phase I clinical trial of LC1 has been initiated.
CLL cells are also induced to apoptosis by two drugs that target the NF-κB pathway in distinct ways; BAY117082, an Ikk inhibitor, and Kamebakaurin, which blocks DNA binding by p50. The Ikk inhibitor BMS-345541 also induces selective killing of CLL cells, accompanied by a decrease in constitutively active NF-κB.
John 6:3-4. 2nd Passover
Then Jesus went up on a mountainside and sat down with his disciples. The Jewish Passover Festival was near.
Some have identified the 'mountainside' with the modern Golan Heights. Jesus' motive was a time alone with his disciples for teaching.
This was presumably the second passover of Jesus' ministry. It is difficult for us to appreciate the significance of the Passover to the 1st century Jew. It was both a time of liberation like the Fourth of July in the USA or the Battle of the Boyne in Northern Ireland and a time of great Spiritual significance. The paschal lamb was slain and eaten to unite the Israelites with their Savior. Following the Exodus, manna in the desert became the bread that suststained them and later in this chapter Jesus will identify himself as the true bread of life. Interestingly the Christian Church did not keep up the Passover after it was established, but continued the symbolism of eating bread to remember the sacrifice of Jesus.
Some have identified the 'mountainside' with the modern Golan Heights. Jesus' motive was a time alone with his disciples for teaching.
This was presumably the second passover of Jesus' ministry. It is difficult for us to appreciate the significance of the Passover to the 1st century Jew. It was both a time of liberation like the Fourth of July in the USA or the Battle of the Boyne in Northern Ireland and a time of great Spiritual significance. The paschal lamb was slain and eaten to unite the Israelites with their Savior. Following the Exodus, manna in the desert became the bread that suststained them and later in this chapter Jesus will identify himself as the true bread of life. Interestingly the Christian Church did not keep up the Passover after it was established, but continued the symbolism of eating bread to remember the sacrifice of Jesus.
Thomas Bayes
I have started a book by Sharon Bertsch McGrayne entitled The theory that would not die. It is about Bayesian statistics, about which I know next to nothing, but which I am told were important to crack the Enigma code during the second world war, hunted down Russian submarines and have recently become respectable following two centuries of controversy.
My son works in central London close to the Dissenters Cemetery where the Rev Thomas Beyes, Fellow of the Royal Society and amateur mathematician, is buried. He also lives in Tunbridge Wells where Bayes was a Presbyterian minister, so my interest is raised. Since my son's job is to do with statistics I am ensnared.
As far as I can tell Bayesian statistics might be a short cut for those statistical imponderables endemic in very large clinical trials; they allow you to change your assumptions as you accumulate data. The purists insist that you don't look at your data until you cross a pre-determined threshold and I remember orthodox statisticians dismissing Bayes with contempt. So I will be interested to read the book. I am only on page 21 and already Bayes has been replaced as the hero by Frenchman Pierre Simon Laplace.
My son works in central London close to the Dissenters Cemetery where the Rev Thomas Beyes, Fellow of the Royal Society and amateur mathematician, is buried. He also lives in Tunbridge Wells where Bayes was a Presbyterian minister, so my interest is raised. Since my son's job is to do with statistics I am ensnared.
As far as I can tell Bayesian statistics might be a short cut for those statistical imponderables endemic in very large clinical trials; they allow you to change your assumptions as you accumulate data. The purists insist that you don't look at your data until you cross a pre-determined threshold and I remember orthodox statisticians dismissing Bayes with contempt. So I will be interested to read the book. I am only on page 21 and already Bayes has been replaced as the hero by Frenchman Pierre Simon Laplace.
Monday, July 25, 2011
Akt actions
We think that constitutively activated PTKs may contribute to PI-3k activation, because the Syk inhibitor, R406, induced CLL apoptosis and decreased phosphorylation of Akt and its targets Gsk3β and FoxO3a. However, constitutive PI-3k activity in CLL cells may also result from the phosphorylation and inactivation of Pten phosphatase by casein kinase 2 (Ck2), which negatively modulates PI-3k signalling by degrading PIP3 to PIP2. Ck2 contributes to oncogenesis by blockade of apoptosis and elevated expression of CSNK2A1 transcripts correlates with poor prognosis in CLL.
In T cell leukaemias, Ck2 inactivates Pten via phosphorylation of its C-terminus, resulting in the hyperactivation of PI-3k signalling. Ck2 activity and Pten phosphorylation were strikingly elevated in CLL cells relative to normal mononuclear cells or lymphocytes. Inhibition of Ck2 resulted in decreased phosphorylation of the Pten C-terminus and of apoptotic death.
It is unclear whether the implied anti-apoptotic actions of PI-3k are mediated via activation of Akt. Constitutively phosphorylated (i.e. activated) Akt was not found in some studies of CLL cells, although its activation was dramatically increased, for example by ligation of cell-surface CD160 or of CXCR4. In contrast, phosphorylated Akt was detected in CLL extracts in other studies. These conflicting data may result from the different methodologies used. Barragan et al reported that spontaneously activated Akt was detectable in fresh but not cryopreserved CLL cells, whereas Zhuang et al suggested that harsh extraction procedures were required for the detection of active Akt. Akt may promote CLL cell survival by blocking the Gsk3β-mediated proteasomal degradation of Mcl-1 and inhibition of Akt activation by the highly selective inhibitor Akt –I-1/2 resulted in apoptosis that was preceded by a decline in Mcl-1.
Targeted expression of the TCL1A gene within B cells of transgenic mice results in a disease resembling aggressive CLL. High TCL1 expression by CLL cells is predictive of a poor outcome and overexpression may be the result of decreased levels of the microRNAs mir-29 and miR-181. TCL1 is a co-activator of Akt and growth stimulation following ligation of the BCR correlates with TCL1 levels and with the kinetics of recruitment of Akt to the receptor complex. The high expression of TCL1 may contribute to aggressive disease by facilitating Akt activation following BCR stimulation.
In T cell leukaemias, Ck2 inactivates Pten via phosphorylation of its C-terminus, resulting in the hyperactivation of PI-3k signalling. Ck2 activity and Pten phosphorylation were strikingly elevated in CLL cells relative to normal mononuclear cells or lymphocytes. Inhibition of Ck2 resulted in decreased phosphorylation of the Pten C-terminus and of apoptotic death.
It is unclear whether the implied anti-apoptotic actions of PI-3k are mediated via activation of Akt. Constitutively phosphorylated (i.e. activated) Akt was not found in some studies of CLL cells, although its activation was dramatically increased, for example by ligation of cell-surface CD160 or of CXCR4. In contrast, phosphorylated Akt was detected in CLL extracts in other studies. These conflicting data may result from the different methodologies used. Barragan et al reported that spontaneously activated Akt was detectable in fresh but not cryopreserved CLL cells, whereas Zhuang et al suggested that harsh extraction procedures were required for the detection of active Akt. Akt may promote CLL cell survival by blocking the Gsk3β-mediated proteasomal degradation of Mcl-1 and inhibition of Akt activation by the highly selective inhibitor Akt –I-1/2 resulted in apoptosis that was preceded by a decline in Mcl-1.
Targeted expression of the TCL1A gene within B cells of transgenic mice results in a disease resembling aggressive CLL. High TCL1 expression by CLL cells is predictive of a poor outcome and overexpression may be the result of decreased levels of the microRNAs mir-29 and miR-181. TCL1 is a co-activator of Akt and growth stimulation following ligation of the BCR correlates with TCL1 levels and with the kinetics of recruitment of Akt to the receptor complex. The high expression of TCL1 may contribute to aggressive disease by facilitating Akt activation following BCR stimulation.
Judi Dench box set
Recently we watched a series of BBC plays starring Judi Dench. They date from 1973 to 1991 when she was going through her 'fat' phase. Voluptuous she might have been but since in each part she was called on to play the sexual attraction, I can hardly say that it worked.
The three plays were "Amelie", the Feydeau farce, translated and adapted by Caryl Brahams and Ned Sherrin and starring Patrick Cargill, Bill Fraser and Helen Cherry;
"Make and Break" by Michael Frayn and starring Robert Hardy, Martin Jarvis, Ronald Hines and Frank Windsor; and "Absolute Hell" by Anthony Ackland with Bill Nighy, Charles Gray, Betty Marsden, Francesca Annis, Anthony Calf, Nathaniel Parker, Ronald Pickup and Ray Winstone.
I am afraid I was not happy with any of them. I thought that they were an illustration of the book of Ecclesiastes - Life without God and the title of the third play gave it away - Absolute Hell.
The farce was just silly. Even in 1973, Judi Dench was 39 and no oil painting and too old for the lady's maid who is supposedly attracting a plethora of lovers. The Michael Frayn is a clever play about a workaholic boss who is only interested in making money and prepared to indulge in shady practices to succeed. He is provided by Frayne with opportunities to change. There is an evangelical Christian who witnesses to him. He might have been talking Swahili. The boss just doesn't recognize the language. He is also provided with a Catholic conscience in the Ronald Hines character, but he continually hedges around it and eventually has what he fears is a heart attack. When it proves to be a false alarm he is back to his wicked ways but his conscience has died of fright.
"Absolute Hell" is set in a 1945 night club in London. The characters indulge in drunkenness, bitchiness and mechanical and illicit sex. The title describes the action.
This is a box set. The first four plays are the same play from the point of view of each different character, "Talking to a stranger". They were so bad I couldn't finish them. There is Chekhov's "The Cherry Orchard" and Ibsen's "Ghosts" and two modern plays, "Can you hear me thinking" and "Going gently" still to watch.
The three plays were "Amelie", the Feydeau farce, translated and adapted by Caryl Brahams and Ned Sherrin and starring Patrick Cargill, Bill Fraser and Helen Cherry;
"Make and Break" by Michael Frayn and starring Robert Hardy, Martin Jarvis, Ronald Hines and Frank Windsor; and "Absolute Hell" by Anthony Ackland with Bill Nighy, Charles Gray, Betty Marsden, Francesca Annis, Anthony Calf, Nathaniel Parker, Ronald Pickup and Ray Winstone.
I am afraid I was not happy with any of them. I thought that they were an illustration of the book of Ecclesiastes - Life without God and the title of the third play gave it away - Absolute Hell.
The farce was just silly. Even in 1973, Judi Dench was 39 and no oil painting and too old for the lady's maid who is supposedly attracting a plethora of lovers. The Michael Frayn is a clever play about a workaholic boss who is only interested in making money and prepared to indulge in shady practices to succeed. He is provided by Frayne with opportunities to change. There is an evangelical Christian who witnesses to him. He might have been talking Swahili. The boss just doesn't recognize the language. He is also provided with a Catholic conscience in the Ronald Hines character, but he continually hedges around it and eventually has what he fears is a heart attack. When it proves to be a false alarm he is back to his wicked ways but his conscience has died of fright.
"Absolute Hell" is set in a 1945 night club in London. The characters indulge in drunkenness, bitchiness and mechanical and illicit sex. The title describes the action.
This is a box set. The first four plays are the same play from the point of view of each different character, "Talking to a stranger". They were so bad I couldn't finish them. There is Chekhov's "The Cherry Orchard" and Ibsen's "Ghosts" and two modern plays, "Can you hear me thinking" and "Going gently" still to watch.
John 6: 1-2. Everybody wants healing.
Some time after this, Jesus crossed to the far shore of the Sea of Galilee (that is, the Sea of Tiberias), and a great crowd of people followed him because they saw the signs he had performed by healing the sick.
People always chase after the spectacular, especially if it involves healing. For Jesus the healing miracles were only a sign - that all things would be restored to the state before the Fall when there was no sickness; that the curse would be removed. It was a sign of the fulfilment of Isaiah 53 by the Christ. Yet people want the sign not the substance. Do they want to be cleansed within?
I saw in the newspaper today that slimmers seldom go back to their former svelte body shape. They still fatten up again when they stop dieting. So it is with sinners. Only the Holy Spirit wreaks a real change.
All those who were healed; even those who were raised from the dead had to die again. Undoubtedly Jesus had compassion on those who were suffering just as any modern doctor would, but there were plenty of sick people in Israel and Judah who were not healed when Jesus walked the land. It was not the main purpose of his time on earth. I hope that had I met him in Jerusalem, my request to him would not have been, "Cure my cancer," but "save my soul."
Today we have grand healing missions. I have to say that I think their priority is misplaced.
People always chase after the spectacular, especially if it involves healing. For Jesus the healing miracles were only a sign - that all things would be restored to the state before the Fall when there was no sickness; that the curse would be removed. It was a sign of the fulfilment of Isaiah 53 by the Christ. Yet people want the sign not the substance. Do they want to be cleansed within?
I saw in the newspaper today that slimmers seldom go back to their former svelte body shape. They still fatten up again when they stop dieting. So it is with sinners. Only the Holy Spirit wreaks a real change.
All those who were healed; even those who were raised from the dead had to die again. Undoubtedly Jesus had compassion on those who were suffering just as any modern doctor would, but there were plenty of sick people in Israel and Judah who were not healed when Jesus walked the land. It was not the main purpose of his time on earth. I hope that had I met him in Jerusalem, my request to him would not have been, "Cure my cancer," but "save my soul."
Today we have grand healing missions. I have to say that I think their priority is misplaced.
Health update
I am having a day of fasting today. Yesterday I had a severe attack of colic in the evening without adequate explanation. Possibly it was having a very fatty pudding after lunch on Saturday, though I can't be sure. Certainly, I feel better this morning for missing a meal yesterday, so I think it will just be liquids for me today. I'm carrying enough adipose tissue not to miss the calories.
I still lack the energy that I had before all this started and the 2mg of dexamethasone that I take have shifted my shape a little. One of the reasons that I chose a new wrist watch as my wedding anniversary present this week was that the circumference of my wrists has shrunk. I will be glad to get off the steroids if that is possible.
I still lack the energy that I had before all this started and the 2mg of dexamethasone that I take have shifted my shape a little. One of the reasons that I chose a new wrist watch as my wedding anniversary present this week was that the circumference of my wrists has shrunk. I will be glad to get off the steroids if that is possible.
The signaling background to CAL-101

Time to remind you of the diagram. If you follow the middle passage of Lyn and Syk activation, the PI-3K δ isoform, which is restricted to hematopoietic cells, plays a key role in B cell receptor signalling. BCR engagement activates PI-3Kδ, which adds an additional phosphate group to PIP2, generating phosphatidylinositol 3,4,5- trisphosphate (PIP3).
The Akt protein kinase and phosphoinositide-dependent protein kinase 1 (Pdk1) contain pleckstrin homology domains that mediate their binding to membrane-localized PIP3. The resulting juxtaposition of the two kinases allows activation of AKT by Pdk1-mediated phosphorylation. Activated Akt blocks apoptosis by multiple pathways.
Since we can identify activating mutations of PI-3k genes this pathway is very important in cancer. We also know that the PI-3k/Akt pathway is downregulated by the action of the phospholipase and tensin homolog (Pten), which dephosphorylates PIP3 to PIP2, thus terminating the ability of PIP3 to activate Akt. PTEN is therefore a tumour suppressor gene, whose loss results in aberrant activation of the PI-3k/Akt pathway in malignant cells.
Constitutive PI-3k activity is significantly greater in CLL cells than in normal B cells. Inhibition of PI-3k by LY294002 results in apoptosis of CLL cells. LY294002 lacks isoform specificity and is likely to cause unacceptable toxicities, especially due to hypoglycaemia resulting from broad inhibition of PI-3k isoforms. Isoform-selective inhibitors of both PI-3k and Akt are in clinical trials in solid tumors. The PI-3Kδ isoform is relatively selective for hematopoietic cells and is elevated approximately three-fold in CLL cells compared to normal B cells. PI-3kδ inhibition by the isoform-selective inhibitor CAL-101 induces apoptosis of CLL cells and is in quite advanced clinical trials. PI-103, an inhibitor that targets both PI-3k and its downstream target mTorc1, blocks the increase of Akt phosphorylation induced by CXCL12 and enhanced apoptosis induction by fludarabine.
I'm sure that those who have read the CAL-101 article will find this all too familiar, but here it is in the raw.
Sunday, July 24, 2011
Pretty Polly Oliver
I phoned my 91 year old mother this afternoon. She had been trying to remember the words to Polly Oliver which I asked her about last weekend. I had eventually found them on the Internet, but the words she remembered today were quite different to those on the net so I have written them down here for posterity's sake. The tune is the same though.
Oh Pretty Polly Oliver, one hot summer's day
To Milvern to market was making her way
With a basket of butter and eggs by the score
And cream from the dairy, a gallon or more.
Her basket was heavy so Polly sat down
To rest by the wayside a mile from the town.
She fell fast asleep there and woke with a scream;
Her basket was empty and spilt was her cream.
"Ah me!" cried Polly Oliver, "What now shall I do?
My master will beat me 'til I'm black and blue.
Kind powers befriend me and lend me your aid,
Take pity upon me, while fortunes are made."
From Bath came that morning the Earl riding by.
He sprang from his stirrup when he heard Polly cry.
Her story she told him; all of the strife.
"Oh pretty Polly Oliver, I'll make you my wife."
The day they were wedded she made him a cake
Of eggs cream and butter for fond memory's sake.
And every year after she made him the same
And that's how Bartholemews have come by their name.
Oh Pretty Polly Oliver, one hot summer's day
To Milvern to market was making her way
With a basket of butter and eggs by the score
And cream from the dairy, a gallon or more.
Her basket was heavy so Polly sat down
To rest by the wayside a mile from the town.
She fell fast asleep there and woke with a scream;
Her basket was empty and spilt was her cream.
"Ah me!" cried Polly Oliver, "What now shall I do?
My master will beat me 'til I'm black and blue.
Kind powers befriend me and lend me your aid,
Take pity upon me, while fortunes are made."
From Bath came that morning the Earl riding by.
He sprang from his stirrup when he heard Polly cry.
Her story she told him; all of the strife.
"Oh pretty Polly Oliver, I'll make you my wife."
The day they were wedded she made him a cake
Of eggs cream and butter for fond memory's sake.
And every year after she made him the same
And that's how Bartholemews have come by their name.
John 6:1-15. The feeding of the five thousand
We are back in Galilee again. This is the only miracle that is recorded in all four gospels.
We might wonder why. Perhaps it is something to do with the fact that in our age, famine and hunger is so widespread while there is clearly food to go around in the world. At the current time there is famine in the horn of Africa. We might speculate why this is so. Corruption in government, war, false religion, climate change, greed, the result of the credit crunch, racism; all will have their favorite cause, but none of them remedies the situation. When there was famine in Abraham's promised land there was corn in Egypt. Joseph had been sent on ahead to rescue the nation of Israel (as it became).
The truth is that there is food enough to feed the starving and we buy play stations and iPhones. If you haven't given yet of your excess when are you going to start?
We might wonder why. Perhaps it is something to do with the fact that in our age, famine and hunger is so widespread while there is clearly food to go around in the world. At the current time there is famine in the horn of Africa. We might speculate why this is so. Corruption in government, war, false religion, climate change, greed, the result of the credit crunch, racism; all will have their favorite cause, but none of them remedies the situation. When there was famine in Abraham's promised land there was corn in Egypt. Joseph had been sent on ahead to rescue the nation of Israel (as it became).
The truth is that there is food enough to feed the starving and we buy play stations and iPhones. If you haven't given yet of your excess when are you going to start?
Chlorambucil and nilotinib for end stage CLL?
A significant problem in treating CLL is that although patients often initially respond to conventional treatment they eventually become resistant to the drugs. While fludarabine based chemotherapy has become a commonly used therapy in CLL, chlorambucil (CLB) results in equivalent survival in older patients.
While we all know about TP53 deletions and mutations as causes of drug resistance in CLL, there are other mechanisms that are important.
CLB cytotoxicity is mediated by the introduction of DNA interstrand cross-links (ICLs). Interstrand crosslinking agents may induce double strand breaks (DSBs) as an intermediate step during ICL repair. Repair of CLB-induced DNA damage in CLL lymphocytes has been shown to be mediated by either nonhomologous end-joining (NHEJ) or homologous recombinational repair (HRR).
In other words alkylating agents like CLB damage cells by forming irregular links between the strands of DNA and as an intermediate step can cause simple breaks in the DNA strands. There are at least two mechanisms by which this DNA damage can be repaired.
Resistance to CLB treatment correlates with Rad51-related HRR or DNA-dependent protein kinase (DNA-PK) activity (a major component of NHEJ) in CLL lymphocytes. The HRR process is modulated by c-abl-mediated phosphorylation of Rad51. c-abl is important for normal B-cell development and is overexpressed in CLL-lymphocytes compared with normal B cells; the isoform 1b is involved in protection from apoptosis. CLB stimulates c-abl phosphorylation and activated c-abl results in phosphorylation of Rad51. Imatinib inhibition of c-abl results in decreased CLB-mediated c-abl phosphorylation and decreased CLB-mediated Rad51 phosphorylation with resultant sensitization of CLL lymphocytes to CLB.
As we have seen in the signaling series c-abl is an important molecule in CLL and I have previously written about imatinib (Gleevec) in CLL. In this month's Leukemia Research a paper from Canada looks again at CLB resistance and c-abl.
In this study they have demonstrated that the potent c-abl inhibitor nilotinib, when compared to imatinib, resulted in a greater synergistic effect with CLB in most of the CLL lymphocyte samples. Also, no statistically significant associations or differences were found between nilotinib or imatinib-mediated sensitization to CLB and the clinical status, Rai stage, Binet stage, ZAP70 expression, somatic mutations in IgVH or c-abl expression.
c-abl has the potential to become auto-phosphorylated on tyrosine and this correlates with increased activity. Biochemical assays with purified recombinant abl kinase showed that nilotinib is a 20–30-fold more potent inhibitor than imatinib for c-abl. Previously they showed that c-abl inhibition by imatinib resulted in sensitization to CLB in vitro. In support of these results, a phase I trial of imatinib and chlorambucil resulted in a 45% response rate in a heavily pretreated CLL patient population. Based on these results, they hypothesized that nilotinib in combination with CLB may be useful to improve therapy for CLL. In this in vitro study, nilotinib inhibited c-abl and sensitized primary B-CLL lymphocytes to CLB more than imatinib. The cytotoxicities of various drug combinations, obtained by MTT assay, were confirmed by analysis of the apoptotic pathway. Apoptosis induced by imatinib in cell lines of lymphatic origin is based on the cleavage of caspase-3. In the current study, They demonstrated that nilotinib potentiated CLB-induced caspase-3 activation to promote apoptotic cell death in primary CLL lymphocytes.
They have previously demonstrated that inhibition of DNA repair sensitizes CLL-lymphocytes to CLB. Down-regulation of either HRR or NHEJ pathways using specific inhibitors of c-abl (imatinib) or DNA-PK (NU7026/NU7441) respectively, resulted in an increase in CLB-induced cytotoxicity associated with decreased DNA repair. Evaluation of the HRR pathway confirmed their previous data showing that imatinib inhibited CLB-induced Rad51 foci formation. Surprisingly, in spite of the fact that nilotinib inhibits c-abl with higher potency than imatinib in CLL lymphocytes they did not find any differences between nilotinib and imatinib inhibition of CLB-induced Rad51 foci formation.
While one factor may be the sensitivity of the assay, their results strongly suggest that inhibition of c-abl with resulting inhibition of HRR can stimulate NHEJ. To evaluate if HRR inhibition can be compensated by the upregulation of the NHEJ pathway, they assessed the phosphorylation status of DNA-PK in CLL lymphocytes. In CLL lymphocyte samples where both c-abl inhibitors demonstrated similar sensitization to CLB, there was an increase in DNA-PK auto-phosphorylation(reflecting the activity of the kinase) induced by inhibition of CLB-induced HRR repair.
Furthermore, simultaneous inhibition of both the HRR (with a c-abl inhibitor; i.e. nilotinib or imatinib) and the NHEJ (with the DNA-PK inhibitor, NU7026) pathways potentiated the synergistic effect of either inhibitor alone on CLB cytotoxicity in CLL lymphocytes and was associated with an increase in CLB-induced DNA damage at 24 h and decreased DNA repair. The effect on CLB cytotoxicity in the presence of DNA-PK inhibition was more pronounced with the more potent c-abl inhibitor, nilotinib.
In conclusion, they have demonstrated a dynamic interaction between two major DNA repair pathways, HRR and NHEJ in CLL lymphocytes in response to CLB-induced DNA damage which should have important clinical implications.
The bottom line is that the the combination of nilotinib plus chlorambucil might be even better than Gleevec and chlorambucil for end-stage, drug resustant CLL. It wil be realtively expensive, but it does provide a possible last resort (oral) treatment. Clinical trials should begin shortly.
While we all know about TP53 deletions and mutations as causes of drug resistance in CLL, there are other mechanisms that are important.
CLB cytotoxicity is mediated by the introduction of DNA interstrand cross-links (ICLs). Interstrand crosslinking agents may induce double strand breaks (DSBs) as an intermediate step during ICL repair. Repair of CLB-induced DNA damage in CLL lymphocytes has been shown to be mediated by either nonhomologous end-joining (NHEJ) or homologous recombinational repair (HRR).
In other words alkylating agents like CLB damage cells by forming irregular links between the strands of DNA and as an intermediate step can cause simple breaks in the DNA strands. There are at least two mechanisms by which this DNA damage can be repaired.
Resistance to CLB treatment correlates with Rad51-related HRR or DNA-dependent protein kinase (DNA-PK) activity (a major component of NHEJ) in CLL lymphocytes. The HRR process is modulated by c-abl-mediated phosphorylation of Rad51. c-abl is important for normal B-cell development and is overexpressed in CLL-lymphocytes compared with normal B cells; the isoform 1b is involved in protection from apoptosis. CLB stimulates c-abl phosphorylation and activated c-abl results in phosphorylation of Rad51. Imatinib inhibition of c-abl results in decreased CLB-mediated c-abl phosphorylation and decreased CLB-mediated Rad51 phosphorylation with resultant sensitization of CLL lymphocytes to CLB.
As we have seen in the signaling series c-abl is an important molecule in CLL and I have previously written about imatinib (Gleevec) in CLL. In this month's Leukemia Research a paper from Canada looks again at CLB resistance and c-abl.
In this study they have demonstrated that the potent c-abl inhibitor nilotinib, when compared to imatinib, resulted in a greater synergistic effect with CLB in most of the CLL lymphocyte samples. Also, no statistically significant associations or differences were found between nilotinib or imatinib-mediated sensitization to CLB and the clinical status, Rai stage, Binet stage, ZAP70 expression, somatic mutations in IgVH or c-abl expression.
c-abl has the potential to become auto-phosphorylated on tyrosine and this correlates with increased activity. Biochemical assays with purified recombinant abl kinase showed that nilotinib is a 20–30-fold more potent inhibitor than imatinib for c-abl. Previously they showed that c-abl inhibition by imatinib resulted in sensitization to CLB in vitro. In support of these results, a phase I trial of imatinib and chlorambucil resulted in a 45% response rate in a heavily pretreated CLL patient population. Based on these results, they hypothesized that nilotinib in combination with CLB may be useful to improve therapy for CLL. In this in vitro study, nilotinib inhibited c-abl and sensitized primary B-CLL lymphocytes to CLB more than imatinib. The cytotoxicities of various drug combinations, obtained by MTT assay, were confirmed by analysis of the apoptotic pathway. Apoptosis induced by imatinib in cell lines of lymphatic origin is based on the cleavage of caspase-3. In the current study, They demonstrated that nilotinib potentiated CLB-induced caspase-3 activation to promote apoptotic cell death in primary CLL lymphocytes.
They have previously demonstrated that inhibition of DNA repair sensitizes CLL-lymphocytes to CLB. Down-regulation of either HRR or NHEJ pathways using specific inhibitors of c-abl (imatinib) or DNA-PK (NU7026/NU7441) respectively, resulted in an increase in CLB-induced cytotoxicity associated with decreased DNA repair. Evaluation of the HRR pathway confirmed their previous data showing that imatinib inhibited CLB-induced Rad51 foci formation. Surprisingly, in spite of the fact that nilotinib inhibits c-abl with higher potency than imatinib in CLL lymphocytes they did not find any differences between nilotinib and imatinib inhibition of CLB-induced Rad51 foci formation.
While one factor may be the sensitivity of the assay, their results strongly suggest that inhibition of c-abl with resulting inhibition of HRR can stimulate NHEJ. To evaluate if HRR inhibition can be compensated by the upregulation of the NHEJ pathway, they assessed the phosphorylation status of DNA-PK in CLL lymphocytes. In CLL lymphocyte samples where both c-abl inhibitors demonstrated similar sensitization to CLB, there was an increase in DNA-PK auto-phosphorylation(reflecting the activity of the kinase) induced by inhibition of CLB-induced HRR repair.
Furthermore, simultaneous inhibition of both the HRR (with a c-abl inhibitor; i.e. nilotinib or imatinib) and the NHEJ (with the DNA-PK inhibitor, NU7026) pathways potentiated the synergistic effect of either inhibitor alone on CLB cytotoxicity in CLL lymphocytes and was associated with an increase in CLB-induced DNA damage at 24 h and decreased DNA repair. The effect on CLB cytotoxicity in the presence of DNA-PK inhibition was more pronounced with the more potent c-abl inhibitor, nilotinib.
In conclusion, they have demonstrated a dynamic interaction between two major DNA repair pathways, HRR and NHEJ in CLL lymphocytes in response to CLB-induced DNA damage which should have important clinical implications.
The bottom line is that the the combination of nilotinib plus chlorambucil might be even better than Gleevec and chlorambucil for end-stage, drug resustant CLL. It wil be realtively expensive, but it does provide a possible last resort (oral) treatment. Clinical trials should begin shortly.
Saturday, July 23, 2011
Lyn and Syk activate resistance pathways
The generation of phosphotyrosine residues by Lyn and Syk results in the activation of multiple pathways. Key mechanisms pertinent to cell survival are briefly summarized here.
Activation of Phospho lipase c gamma2 (Plc gamma 2) following BCR engagement results in cleavage of phosphatidylinositol 4,5-bisphosphate (PIP2) and the generation of two second messenger molecules, diacylglycerol (DAG) and inositol 1,4,5-trisphosphate (IP3). DAG binding activates Pkcβ, thus blocking cell death by upregulating transcription of anti-apoptotic genes via nuclear factor-κB (NF-κB).
Binding of IP3 to Ca2+ channels releases Ca2+ ions stored in the endoplasmic reticulum. Released Ca2+ binds calmodulin (Cam) and the Ca2+/Cam complex activates the phosphatase, calcineurin. Activation of the transcription factor NFAT by calcineurin-mediated dephosphorylation results in transcription of several genes including those of IL-2, IL-4 and gamma-interferon, which block apoptosis of CLL cells.
Pkcβ overexpression correlates with poor prognosis in CLL and PRKCB deletion prevents development of CLL-like disease in Eμ-TCL1 transgenic mice, suggesting a key role in CLL pathogenesis. Enzastaurin, an inhibitor targeting both Pkcβ and Akt, induced apoptosis of CLL cells but not of T cells in vitro. A phase I study of this agent has started.
It gets more complicated still. The thing to remember about cell signaling is that there are many back-up systems and blocking one pathway may mean that back-up is called into play. Multiple drugs are probably going to be necessary. In this respect CML and Gleevec are exceptions to the general rule.
Activation of Phospho lipase c gamma2 (Plc gamma 2) following BCR engagement results in cleavage of phosphatidylinositol 4,5-bisphosphate (PIP2) and the generation of two second messenger molecules, diacylglycerol (DAG) and inositol 1,4,5-trisphosphate (IP3). DAG binding activates Pkcβ, thus blocking cell death by upregulating transcription of anti-apoptotic genes via nuclear factor-κB (NF-κB).
Binding of IP3 to Ca2+ channels releases Ca2+ ions stored in the endoplasmic reticulum. Released Ca2+ binds calmodulin (Cam) and the Ca2+/Cam complex activates the phosphatase, calcineurin. Activation of the transcription factor NFAT by calcineurin-mediated dephosphorylation results in transcription of several genes including those of IL-2, IL-4 and gamma-interferon, which block apoptosis of CLL cells.
Pkcβ overexpression correlates with poor prognosis in CLL and PRKCB deletion prevents development of CLL-like disease in Eμ-TCL1 transgenic mice, suggesting a key role in CLL pathogenesis. Enzastaurin, an inhibitor targeting both Pkcβ and Akt, induced apoptosis of CLL cells but not of T cells in vitro. A phase I study of this agent has started.
It gets more complicated still. The thing to remember about cell signaling is that there are many back-up systems and blocking one pathway may mean that back-up is called into play. Multiple drugs are probably going to be necessary. In this respect CML and Gleevec are exceptions to the general rule.
What has been happening in South Sudan?
Phone hacking and the Greek economy have dominated the newspapers in the UK but there have been other things happening.
One Christian is martyred every 5 minutes according to Italian sociologist, Lassimo Introvigne. Where is it happening?
One place has been in the civil war between North and South Sudan where thousands were killed and as recently as last month the war was continuing in South Kordofan. Although South Kordofan is part of north Sudan, it has strong ties with the South and their struggle for independence. Ahmed Haroun of the north Sudan’s ruling National Congress Party was declared winner of the state’s gubernatorial election in May, an outcome which the Sudan's People's Liberation Movement strongly disputes, citing claims of vote rigging. Ahmed Haroun is a war lord heavily implicated in the atrocities in Darfur and is under indictment by the War Crimes Tribunal.
On June 5th, Arnu Yusuf, the SPLM’s secretary general for information and communication in South Kordofan State, told the Sudan Tribune that Sudan Armed Forces (SAF) of north Sudan carried out an attack on their premises and a house belonging to the deputy chairperson of the SPLM’s northern sector, Abdel Aziz Adam El-Hilu. “The Sudan Armed Forces and their police staged an attack directed at our premises today. They wanted to forcefully disarm soldiers guarding our premises,” said Yusuf.
He went on to claim that 14 members of SAF and three armed guards from the SPLA, the SPLM’s military wing, were killed in the clashes. “We have lost three comrades. Two others sustained injuries and the fighting is continuing”, says Yusuf, adding that they are determined to defend themselves.
The SPLM official denied that the fighting which took place today was initiated by armed elements associated with the SPLM. “Our people did not initiate any fighting. The Sudan Armed Forces launched a direct attack on our premises as part of the offensive operation. They started attacking villages on Sunday through Monday without success. They lost in Talodi and in Miri. They also lost the fight in Umm Dorien, so they decided to resume it in town this morning”, said Yusuf, who declined to indicate his whereabouts.
Fighting in the flashpoint state erupted on Sunday, 5 June, as SAF moved into the center of Kadugli town following an attack by unidentified gunmen on a police station in the area. Reliable sources, who wish to retain their anonymity, informed Sudan Tribune that shootings took place at Kadugli airport on Tuesday morning and that the conflict in Kadugli itself involved small arms and rocket propelled grenades. The sources also suggested that the UN Refugee Agency and the World Food Program buildings have been under fire.
The UN office in Kadugli confirmed eruption of a heavy fighting in Kadugli town on Tuesday. Kouider Zerrouk, the spokesperson of the UN Mission in Sudan (UNMIS) said "UNMIS is concerned about the ongoing fighting between the SAF and the SPLA and the deteriorating security situation in Kadugli." The UN official cited a different death toll, saying that only six dead bodies were received in the local police hospital, four of whom were policemen and two civilians.
Meanwhile, another UNMIS spokesperson, Hua Jiang, told reporters that “about 3,000 people [are] taking refuge at the Kadugli police hospital". Musa Kaka, another senior member of the SPLM in the area, in an interview with the Sudan Tribune on Tuesday that the people of the Nuba Mountains would not be the first to initiate the fight, but added that they would not allow themselves to be slaughtered “like chickens” and that they had a right to defend themselves. “Nobody in the Nuba Mountains had intention to fight even though they were denied their rights. Our people are peace-loving people. The people of Nuba Mountains are well known for peace but they cannot allow themselves now to be slaughtered like chickens when they have all rights to defense themselves”, said Kaka.
“We know our people were slaughtered in thousands during the war because we went to the bush with the south to fight against the central which did not want us to live in areas and to have right to equal treatment. It was not our choice to be born as black and in the Nuba Mountains. It was the decision of the God and so we cannot change decision of the creator. We will be here and will remain Nuba Mountains. We will stay in our land dead or alive come what may," he said.
He called on sons and daughters of Nuba Mountains in the SAF not to kill their own people. “I call our people in the government of Khartoum, whether as politicians or in the military, not to accept politics of divide and rule in order to kill our people […] Let us resolve our difference and unite one and the same people”, he appealed.
South Kordofan, which lies on the fault lines between north Sudan and the now independent South Sudan, is one of the country’s heavily militarized regions. It saw fierce fighting during the years of Sudan’s north-south civil wars which ended with the signing of the Comprehensive Peace Agreement in 2005.
One Christian is martyred every 5 minutes according to Italian sociologist, Lassimo Introvigne. Where is it happening?
One place has been in the civil war between North and South Sudan where thousands were killed and as recently as last month the war was continuing in South Kordofan. Although South Kordofan is part of north Sudan, it has strong ties with the South and their struggle for independence. Ahmed Haroun of the north Sudan’s ruling National Congress Party was declared winner of the state’s gubernatorial election in May, an outcome which the Sudan's People's Liberation Movement strongly disputes, citing claims of vote rigging. Ahmed Haroun is a war lord heavily implicated in the atrocities in Darfur and is under indictment by the War Crimes Tribunal.
On June 5th, Arnu Yusuf, the SPLM’s secretary general for information and communication in South Kordofan State, told the Sudan Tribune that Sudan Armed Forces (SAF) of north Sudan carried out an attack on their premises and a house belonging to the deputy chairperson of the SPLM’s northern sector, Abdel Aziz Adam El-Hilu. “The Sudan Armed Forces and their police staged an attack directed at our premises today. They wanted to forcefully disarm soldiers guarding our premises,” said Yusuf.
He went on to claim that 14 members of SAF and three armed guards from the SPLA, the SPLM’s military wing, were killed in the clashes. “We have lost three comrades. Two others sustained injuries and the fighting is continuing”, says Yusuf, adding that they are determined to defend themselves.
The SPLM official denied that the fighting which took place today was initiated by armed elements associated with the SPLM. “Our people did not initiate any fighting. The Sudan Armed Forces launched a direct attack on our premises as part of the offensive operation. They started attacking villages on Sunday through Monday without success. They lost in Talodi and in Miri. They also lost the fight in Umm Dorien, so they decided to resume it in town this morning”, said Yusuf, who declined to indicate his whereabouts.
Fighting in the flashpoint state erupted on Sunday, 5 June, as SAF moved into the center of Kadugli town following an attack by unidentified gunmen on a police station in the area. Reliable sources, who wish to retain their anonymity, informed Sudan Tribune that shootings took place at Kadugli airport on Tuesday morning and that the conflict in Kadugli itself involved small arms and rocket propelled grenades. The sources also suggested that the UN Refugee Agency and the World Food Program buildings have been under fire.
The UN office in Kadugli confirmed eruption of a heavy fighting in Kadugli town on Tuesday. Kouider Zerrouk, the spokesperson of the UN Mission in Sudan (UNMIS) said "UNMIS is concerned about the ongoing fighting between the SAF and the SPLA and the deteriorating security situation in Kadugli." The UN official cited a different death toll, saying that only six dead bodies were received in the local police hospital, four of whom were policemen and two civilians.
Meanwhile, another UNMIS spokesperson, Hua Jiang, told reporters that “about 3,000 people [are] taking refuge at the Kadugli police hospital". Musa Kaka, another senior member of the SPLM in the area, in an interview with the Sudan Tribune on Tuesday that the people of the Nuba Mountains would not be the first to initiate the fight, but added that they would not allow themselves to be slaughtered “like chickens” and that they had a right to defend themselves. “Nobody in the Nuba Mountains had intention to fight even though they were denied their rights. Our people are peace-loving people. The people of Nuba Mountains are well known for peace but they cannot allow themselves now to be slaughtered like chickens when they have all rights to defense themselves”, said Kaka.
“We know our people were slaughtered in thousands during the war because we went to the bush with the south to fight against the central which did not want us to live in areas and to have right to equal treatment. It was not our choice to be born as black and in the Nuba Mountains. It was the decision of the God and so we cannot change decision of the creator. We will be here and will remain Nuba Mountains. We will stay in our land dead or alive come what may," he said.
He called on sons and daughters of Nuba Mountains in the SAF not to kill their own people. “I call our people in the government of Khartoum, whether as politicians or in the military, not to accept politics of divide and rule in order to kill our people […] Let us resolve our difference and unite one and the same people”, he appealed.
South Kordofan, which lies on the fault lines between north Sudan and the now independent South Sudan, is one of the country’s heavily militarized regions. It saw fierce fighting during the years of Sudan’s north-south civil wars which ended with the signing of the Comprehensive Peace Agreement in 2005.
John 5:31-47. The special testimony of John's gospel.
Time for a pause on John's gospel today. Some people want to strip this gospel from the canon of Scripture because it is so different from the synoptics and because it was written so much later; but the real reason is that it so clearly asserts that Jesus is God, and chapter 5 exemplifies this.
However, just what was it that led to Jesus crusifixion? Was it not the charge of blasphemy? When Jesus was accused of making himself out to be God as in, say Luke 22:70 "They all asked, 'Are you then the Son of God?' He replied, 'You are right in saying I am.'"
It could not be plainer than that. So there is no disjunction between the Fourth gospel and the synoptics.
However, just what was it that led to Jesus crusifixion? Was it not the charge of blasphemy? When Jesus was accused of making himself out to be God as in, say Luke 22:70 "They all asked, 'Are you then the Son of God?' He replied, 'You are right in saying I am.'"
It could not be plainer than that. So there is no disjunction between the Fourth gospel and the synoptics.
Norway
Word is coming that the atrocity in Norway has been committed by a right-wing fundamentalist Christian. I begin to feel like a moderate Muslim must feel. However, I will lose no time in condemning any 'Christian' who acts in that way as a vile and wicked sinner who has traduced the name of Jesus. Hitler began as a Christian and turned away fro the teachings of Christ to found his own religion which worshiped some imaginary German character trait. There were many in Norway who followed the traitor, Quisling. They clearly still remain.
My heart and prayers go out to those who have lost loved ones in Oslo and on the island. It is unadulterated wickedness.
My heart and prayers go out to those who have lost loved ones in Oslo and on the island. It is unadulterated wickedness.
How Large a Universe
The Milky Way is a disc some 100,000 light years across that consists of at least 250 billion stars, possibly as many as a trillion. It is 26,000 light years away, and is only one of myriad other galaxies visible in the night sky. We are so alone.
I doubt a God with stars to see
would ever deign to look at me.
Yet if by some mischance he tried
I'd find some secret place to hide
the angry ramblings of my mind
as they are hid, these dark, unkind
and vicious thoughts, by everyone
who fears his precious pride undone.
To Him the darkness is as light,
nothing can hide me from his sight.
A beacon burns for my disgrace
across infinities of space.
The brightest stars are dim beside
the ugly glare of hate and pride,
envy and greed, a fiery flood;
I hide them only in His blood.
I doubt a God with stars to see
would ever deign to look at me.
Yet if by some mischance he tried
I'd find some secret place to hide
the angry ramblings of my mind
as they are hid, these dark, unkind
and vicious thoughts, by everyone
who fears his precious pride undone.
To Him the darkness is as light,
nothing can hide me from his sight.
A beacon burns for my disgrace
across infinities of space.
The brightest stars are dim beside
the ugly glare of hate and pride,
envy and greed, a fiery flood;
I hide them only in His blood.
Friday, July 22, 2011
Signaling: negative regulators of PTKs
Signaling is even more complicated than we have so far discovered. Augmented PTK signaling in CLL cells may also result from decreased expression of negative regulators.
For example, p66Shc blocks Syk phosphorylation, in response to BCR ligation, by competing with p52Shc, the pro-signalling isoform. But p66Shc is strikingly under-expressed in CLL cells relative to normal B cells, with lowest expression in the poor prognosis group. Reconstitution of p66Shc expression by nucleofection (Nucleofection refers to electroporation, a transfection method which enables transfer of nucleic acids such as DNA, RNA, or small interfering RNA into cells) dramatically reduces anti-apoptotic Bcl-2 and Bcl-XL and increases expression of pro-apoptotic Bax and Bak proteins, suggesting that low p66Shc expression skews Bcl-2 family protein expression towards cytoprotection. Patients with Bcl-2/ p66Shc ratios above the median have shorter treatment free intervals and overall survival durations than do patients with ratios below the median, suggesting that p66Shc influences the clinical behaviour of the malignancy. The mechanism underlying low p66Shc expression in CLL is unclear, but epigenetic mechanisms may be involved.
Another example is the leucocyte-associated immunoglobulin-like receptor-1 (Lair-1), which recruits the Shp phosphatase via ITIMs in its cytosolic domain. Deactivation of PTKs by Shp, negatively regulates BCR signalling. Expression of Lair-1 is low in cells from poor risk patients compared to those from better risk patients. Ligation of Lair-1 resulted in a reduction in activity of constitutive Akt and NF-κB in Lair-1-expressing CLL but not in non-expressing isolates, suggesting that decreased expression of Lair-1 contributes to augmented activation of pro-survival pathways in poor-risk patients.
For example, p66Shc blocks Syk phosphorylation, in response to BCR ligation, by competing with p52Shc, the pro-signalling isoform. But p66Shc is strikingly under-expressed in CLL cells relative to normal B cells, with lowest expression in the poor prognosis group. Reconstitution of p66Shc expression by nucleofection (Nucleofection refers to electroporation, a transfection method which enables transfer of nucleic acids such as DNA, RNA, or small interfering RNA into cells) dramatically reduces anti-apoptotic Bcl-2 and Bcl-XL and increases expression of pro-apoptotic Bax and Bak proteins, suggesting that low p66Shc expression skews Bcl-2 family protein expression towards cytoprotection. Patients with Bcl-2/ p66Shc ratios above the median have shorter treatment free intervals and overall survival durations than do patients with ratios below the median, suggesting that p66Shc influences the clinical behaviour of the malignancy. The mechanism underlying low p66Shc expression in CLL is unclear, but epigenetic mechanisms may be involved.
Another example is the leucocyte-associated immunoglobulin-like receptor-1 (Lair-1), which recruits the Shp phosphatase via ITIMs in its cytosolic domain. Deactivation of PTKs by Shp, negatively regulates BCR signalling. Expression of Lair-1 is low in cells from poor risk patients compared to those from better risk patients. Ligation of Lair-1 resulted in a reduction in activity of constitutive Akt and NF-κB in Lair-1-expressing CLL but not in non-expressing isolates, suggesting that decreased expression of Lair-1 contributes to augmented activation of pro-survival pathways in poor-risk patients.
John 5:45-47. Moses accuses.
“But do not think I will accuse you before the Father. Your accuser is Moses, on whom your hopes are set. If you believed Moses, you would believe me, for he wrote about me. But since you do not believe what he wrote, how are you going to believe what I say?”
Here we come to the nub of the Jews' unbelief. It was how they read the books of Moses. Instead of seeing them as pointing forwards to the Messiah, they read them as if they were sufficient unto themselves. The point is not that keeping the Law is sufficient to please God, because nobody can and the temporary plug in the gap, namely the sacrifice of animals can never assuage the anger of God. It takes God himself in the person of Jesus to atone for the sins of the world.
At the last Assize it will not be Jesus who accuses but Moses himself, because as plain as he could be he was still distorted. He pointed forwards to Jesus but the Jews effectively turned him into a demi-god and worshiped the product rather than the Creator; the creation rather than the Redeemer.
Here we come to the nub of the Jews' unbelief. It was how they read the books of Moses. Instead of seeing them as pointing forwards to the Messiah, they read them as if they were sufficient unto themselves. The point is not that keeping the Law is sufficient to please God, because nobody can and the temporary plug in the gap, namely the sacrifice of animals can never assuage the anger of God. It takes God himself in the person of Jesus to atone for the sins of the world.
At the last Assize it will not be Jesus who accuses but Moses himself, because as plain as he could be he was still distorted. He pointed forwards to Jesus but the Jews effectively turned him into a demi-god and worshiped the product rather than the Creator; the creation rather than the Redeemer.
Thursday, July 21, 2011
News from the Barnabas Trust
Muslims Against Crusades are targeting the London borough of Waltham Forest to be the first “sharia-controlled zone” as part of a new “Islamic Emirates Project”.
The group said,
As part of our Islamic Emirate Project, Waltham Forest is to be the first borough to be targeted for an intense sharia led campaign, introducing the prospect of Islamic law for the Muslim community to abide by.
Waltham Forest is...a borough with a marked Islamic fingerprint; Muslim businesses, mosques and Islamic schools emblazon its streets, making a transition into a thriving Islamic emirate, very real and plausible.
The organisation intends to persuade Muslims in Waltham to self-enforce sharia initially with specially designed leaflets and posters that read, “You are entering a Sharia Controlled Zone
Iran’s Supreme Court has upheld the death penalty for a church pastor convicted of apostasy last year – unless he recants his faith.
Pastor Nadarkhani (33) was arrested in his home city of Rasht, northern Iran, in October 2009 for objecting to the teaching of Islam to Christian children in schools. He was initially charged with protesting, but the charges against him were later changed to apostasy and evangelising Muslims. His wife, Fatemeh Passandideh, was also later arrested, in June 2010, and sentenced to life in prison. Supporters say that this was an attempt to pressurise Pastor Nadarkhani to renounce his faith, but he remained steadfast. Fatemeh was released on appeal in October after four months in prison.
Pastor Nadarkhani was found guilty of apostasy in September 2010; a written confirmation of the death sentence was received on 13 November. Apostasy – or renouncing Islam – is not a crime under Iran’s penal code, but the system does make provision for judges to draw on fatwas and Islamic sources where national law is silent. Islamic law states that an adult male apostate should be given the death sentence. The verdict was based on fatwas by key Iranian religious leaders including the Supreme Leader of Iran, Ali Khamenei. Pastor Nadarkhani, who was born to Muslim parents and is thus considered a Muslim in Islamic tradition, became a Christian aged 19.
The case was tried by the court in Rasht and has now been referred back there. The Supreme Court has asked the Rasht court to re-examine some procedural flaws in the case but has ultimately given local judges the power to decide Pastor Nadarkhani’s fate in October. The outcome seems likely to rest on whether or not he will recant his faith.
His lawyer, Mohammed Ali Dadkhah, a prominent defender of human rights in Iran, is involved in a legal battle of his own. He is appealing a nine-year prison sentence and ten-year ban on practising law or teaching at university for “actions and propaganda against the Islamic regime”.
The decision was strongly condemned by the US State Department, which said:
We are dismayed over reports that the Iranian courts are requiring Youcef Nadarkhani to recant his faith or face the death penalty for apostasy, a charge based on his religious beliefs. If carried out, it would be the first execution for apostasy in Iran since 1990.
There has been no protest by the British Government of any European authorities.
An Egyptian human rights organisation has exposed a highly organised Muslim ring that promotes sexual exploitation and blackmail to force Christian girls to convert to Islam
Egypt4Christ, which monitors the abduction and forced Islamisation of Christian minors, published the findings in a new report last week. It launched an undercover investigation after a church leader in Alexandria reported that a ten-year-old Christian girl had been sexually abused by a 20-year-old Muslim university student.
The group discovered that a highly organised Muslim ring based at a mosque in Alexandria are orchestrating a systematic campaign in which they urge young Muslim males in high school and university to approach Christian girls aged 9-15 and manipulate them through sexual exploitation and blackmail. Named “operation soaking lupin beans” (referring to small dried beans that are soaked until they grow in size before being eaten raw), the plan aims to compromise Christian girls sexually so that they feel defiled and humiliated, forcing them to flee their homes. Conversion to Islam is then used as a “solution” to their problems. The group published the names of those involved in the ring, which includes high-ranking officials and a Salafist leader who is reportedly considering running for president in the forthcoming Egyptian elections.
The problem of the forced conversion of Christian girls, who are then married to Muslim men, is a long-standing one in Egypt. But it has intensified since the January Revolution, with the number of Christian girls affected said to be soaring, amid wider efforts to Islamise the country. One church leader in Cairo estimates that at least 21 young girls have disappeared from his parish since the revolution, while another said that “more than two to three girls disappear everyday in Giza alone”. He added, “The cases that are brought to public attention are few compared to what the numbers actually are.”
Christian activist Mark Ebeid said that the problem has escalated since the revolution because of the emergence of Muslim Salafists, who follow an ultra-conservative, strict and puritanical version of Islam related to Wahhabism, the official state creed of Saudi Arabia. Mr Ebeid said they “believe strongly that converting a Christian Infidel is in some ways like earning a ticket to paradise – not to mention the earthly remuneration they get from the Saudis”.
Christians complain that the military council are not intervening in the problem and they do not get any assistance from the police.
The problem is not unique to Egypt; it is also common in Pakistan, and there have been consistent reports of its occurring in India and Sri Lanka. A Christian girl who has been forced to marry a Muslim man faces a virtually hopeless future, held captive by a family who treat her as nothing more than a slave. In Pakistan and Egypt, the woman’s name and identity is changed, with her Christian religious status being replaced with Islam on her identity card.
The group said,
As part of our Islamic Emirate Project, Waltham Forest is to be the first borough to be targeted for an intense sharia led campaign, introducing the prospect of Islamic law for the Muslim community to abide by.
Waltham Forest is...a borough with a marked Islamic fingerprint; Muslim businesses, mosques and Islamic schools emblazon its streets, making a transition into a thriving Islamic emirate, very real and plausible.
The organisation intends to persuade Muslims in Waltham to self-enforce sharia initially with specially designed leaflets and posters that read, “You are entering a Sharia Controlled Zone
Iran’s Supreme Court has upheld the death penalty for a church pastor convicted of apostasy last year – unless he recants his faith.
Pastor Nadarkhani (33) was arrested in his home city of Rasht, northern Iran, in October 2009 for objecting to the teaching of Islam to Christian children in schools. He was initially charged with protesting, but the charges against him were later changed to apostasy and evangelising Muslims. His wife, Fatemeh Passandideh, was also later arrested, in June 2010, and sentenced to life in prison. Supporters say that this was an attempt to pressurise Pastor Nadarkhani to renounce his faith, but he remained steadfast. Fatemeh was released on appeal in October after four months in prison.
Pastor Nadarkhani was found guilty of apostasy in September 2010; a written confirmation of the death sentence was received on 13 November. Apostasy – or renouncing Islam – is not a crime under Iran’s penal code, but the system does make provision for judges to draw on fatwas and Islamic sources where national law is silent. Islamic law states that an adult male apostate should be given the death sentence. The verdict was based on fatwas by key Iranian religious leaders including the Supreme Leader of Iran, Ali Khamenei. Pastor Nadarkhani, who was born to Muslim parents and is thus considered a Muslim in Islamic tradition, became a Christian aged 19.
The case was tried by the court in Rasht and has now been referred back there. The Supreme Court has asked the Rasht court to re-examine some procedural flaws in the case but has ultimately given local judges the power to decide Pastor Nadarkhani’s fate in October. The outcome seems likely to rest on whether or not he will recant his faith.
His lawyer, Mohammed Ali Dadkhah, a prominent defender of human rights in Iran, is involved in a legal battle of his own. He is appealing a nine-year prison sentence and ten-year ban on practising law or teaching at university for “actions and propaganda against the Islamic regime”.
The decision was strongly condemned by the US State Department, which said:
We are dismayed over reports that the Iranian courts are requiring Youcef Nadarkhani to recant his faith or face the death penalty for apostasy, a charge based on his religious beliefs. If carried out, it would be the first execution for apostasy in Iran since 1990.
There has been no protest by the British Government of any European authorities.
An Egyptian human rights organisation has exposed a highly organised Muslim ring that promotes sexual exploitation and blackmail to force Christian girls to convert to Islam
Egypt4Christ, which monitors the abduction and forced Islamisation of Christian minors, published the findings in a new report last week. It launched an undercover investigation after a church leader in Alexandria reported that a ten-year-old Christian girl had been sexually abused by a 20-year-old Muslim university student.
The group discovered that a highly organised Muslim ring based at a mosque in Alexandria are orchestrating a systematic campaign in which they urge young Muslim males in high school and university to approach Christian girls aged 9-15 and manipulate them through sexual exploitation and blackmail. Named “operation soaking lupin beans” (referring to small dried beans that are soaked until they grow in size before being eaten raw), the plan aims to compromise Christian girls sexually so that they feel defiled and humiliated, forcing them to flee their homes. Conversion to Islam is then used as a “solution” to their problems. The group published the names of those involved in the ring, which includes high-ranking officials and a Salafist leader who is reportedly considering running for president in the forthcoming Egyptian elections.
The problem of the forced conversion of Christian girls, who are then married to Muslim men, is a long-standing one in Egypt. But it has intensified since the January Revolution, with the number of Christian girls affected said to be soaring, amid wider efforts to Islamise the country. One church leader in Cairo estimates that at least 21 young girls have disappeared from his parish since the revolution, while another said that “more than two to three girls disappear everyday in Giza alone”. He added, “The cases that are brought to public attention are few compared to what the numbers actually are.”
Christian activist Mark Ebeid said that the problem has escalated since the revolution because of the emergence of Muslim Salafists, who follow an ultra-conservative, strict and puritanical version of Islam related to Wahhabism, the official state creed of Saudi Arabia. Mr Ebeid said they “believe strongly that converting a Christian Infidel is in some ways like earning a ticket to paradise – not to mention the earthly remuneration they get from the Saudis”.
Christians complain that the military council are not intervening in the problem and they do not get any assistance from the police.
The problem is not unique to Egypt; it is also common in Pakistan, and there have been consistent reports of its occurring in India and Sri Lanka. A Christian girl who has been forced to marry a Muslim man faces a virtually hopeless future, held captive by a family who treat her as nothing more than a slave. In Pakistan and Egypt, the woman’s name and identity is changed, with her Christian religious status being replaced with Islam on her identity card.
Signaling in CLL. Is this how lenalidomide works?
Remember those gene expression profiles of CLL cells that were published in 2001(Klein et al; Rosenwald et al)? Both showed that the mRNA encoding the PTK receptor Ror1 (it stands for receptor tyrosine kinase-like orphan receptor) is overexpressed by CLL cells. Nine years later it was demonstrated that Ror1 protein was expressed by CLL cells but not by normal T or B lymphocytes nor by the majority of adult tissues. There seems to be a link with both Tom Kipps' gene therapy approach and with lenalidomide treatment.
Ror1 levels were remarkably uniform in cells from CLL patients and were independent of IGHV mutation status. Ror1 is engaged by Wnt5a, an interaction that induces NF-κB activity. Wnt5a augments survival of CLL cells and this protection was abolished by anti-Ror1 antisera. These observations, together with the uniform expression of Ror1 in CLL, suggest that it may be a promising candidate for therapeutic targeting. T cells engineered to express chimeric antigen receptors against Ror1 have been constructed. These cells target primary CLL cells in vitro, including rare drug-resistant clones.
Transfection of CD154 into CLL cells ex vivo followed by reinfusion of the transfected cells into patients results in the generation of anti-Ror1 antibodies, suggesting that ectopic expression of CD154 corrects the immune dysfunction characteristic of CLL, thereby facilitates immune responses against Ror1. Treatment of CLL patients with lenalidomide also results in CD154 upregulation. The consequent generation of anti-Ror1 antibodies by a lenalidomide-treated patient may underlie the therapeutic activity of this drug in CLL.
Ror1 levels were remarkably uniform in cells from CLL patients and were independent of IGHV mutation status. Ror1 is engaged by Wnt5a, an interaction that induces NF-κB activity. Wnt5a augments survival of CLL cells and this protection was abolished by anti-Ror1 antisera. These observations, together with the uniform expression of Ror1 in CLL, suggest that it may be a promising candidate for therapeutic targeting. T cells engineered to express chimeric antigen receptors against Ror1 have been constructed. These cells target primary CLL cells in vitro, including rare drug-resistant clones.
Transfection of CD154 into CLL cells ex vivo followed by reinfusion of the transfected cells into patients results in the generation of anti-Ror1 antibodies, suggesting that ectopic expression of CD154 corrects the immune dysfunction characteristic of CLL, thereby facilitates immune responses against Ror1. Treatment of CLL patients with lenalidomide also results in CD154 upregulation. The consequent generation of anti-Ror1 antibodies by a lenalidomide-treated patient may underlie the therapeutic activity of this drug in CLL.
John 5:44. I'm one of the in-crowd!
How can you believe if you accept praise from one another, yet make no effort to obtain praise that comes from the only God?
We begin to see Jesus' insight into the Pharisees. They belong to an inward looking coterie of people who pat each other on the back for their mutual wisdom. Such self-regarding is the direct opposite of the humility that the Christian life commands. Don't we see it today in the arty-set or the media darlings? Belonging to an in-group immediately sets one aside from an out-group. In Romans 2:29, Paul defines a 'true Jew' whose heart has been circumcized as one 'whose praise is not from men but from God'.
How do we measure up in this regard? Are you open to everyone? Are there some people you wouldn't be seen dead with? How is your small group meeting? Is it a mixture of social class, age-range, ethnicity, married and single, income, mature and immature? Being all of one mind is fine as far as the Gospel goes, but we are all coming from different directions in this world and we need the humility to realize this.
We begin to see Jesus' insight into the Pharisees. They belong to an inward looking coterie of people who pat each other on the back for their mutual wisdom. Such self-regarding is the direct opposite of the humility that the Christian life commands. Don't we see it today in the arty-set or the media darlings? Belonging to an in-group immediately sets one aside from an out-group. In Romans 2:29, Paul defines a 'true Jew' whose heart has been circumcized as one 'whose praise is not from men but from God'.
How do we measure up in this regard? Are you open to everyone? Are there some people you wouldn't be seen dead with? How is your small group meeting? Is it a mixture of social class, age-range, ethnicity, married and single, income, mature and immature? Being all of one mind is fine as far as the Gospel goes, but we are all coming from different directions in this world and we need the humility to realize this.
Wednesday, July 20, 2011
Ig paraprotein in CLL. What does it mean?
Several people have asked whether having a paraprotein in the serum influences the outcome in CLL. A paper in Leukemia Research from China addresses this problem.
They studied 133 patients with CLL, 86 male and 47 female, median age at diagnosis 60 (range, 44–84). They identified 27 patients with Ig paraproteinemia (12 with IgG, 12 with IgM, 3 with both IgG and IgM, but none with IgA), frequency of 20.3%. The median level of serum IgG paraprotein was 28.2 g/l (range, 21.0–62.0 g/l), and IgM paraprotein was 18.1 g/l (range, 2.3–49.1 g/l). The serum monoclonal Ig light chain concordant with the monoclonal Ig light chain expressed by the neoplastic cells in all patients with Ig paraproteinemia.
Strong correlations of serum Ig paraprotein with advanced Binet stage, DAT-positivity, high level of Beta2-MG and TK1, absence of IGHV mutations, ZAP-70-positivity, CD38-positivity, and cytogenetic abnormalities of del(17p13) or del(11q22)were observed.
With a median follow-up of 36 months (range, 4–83 months), 13 patients (9.8%) died. The prognostic factors with statistical significance were considered in a multivariate Cox regression analysis, del(17p13) ZAP-70, and IgM paraproteinemia were the variables strongly associated with survival.
Ig paraproteinemia was associated with poor outcome. Six (22.2%) with Ig paraproteinemia died during the observation period (2 with IgG paraprotein, 2 with IgM paraprotein, 2 patients with both IgG and IgM, respectively), whereas among the 106 patients without Ig paraproteinemia, 7 (6.6%) died. Patients with Ig paraproteinemia had significantly shorter survival times than patients without serum Ig paraprotein.
Bernstein and colleagues], in a study of 111 patients, reported that the presence of serum monoclonal protein in patients with CLL was associated with a shorter median
survival: 63 months for patients with CLL with serum Ig paraprotein compared with 103 months for patients without serum Ig paraprotein. However, Yin and colleagues have not confirmed this observation. The unfavorable prognostic significance of serum Ig paraprotein was observed in this study.
The possible explanations of discrepancy in prognostic impact of serum Ig paraprotein might be different therapeutic regimens, shorter clinical follow-up and smaller number of patients. retained their capability of isotype switching, a process independent of immunoglobulin heavy chain gene mutation. As an alternative, these additional M components may represent biclonal or triclonal ymphoproliferative disorders as described in the literature or the development of a subclone within the original tumor cells due to clonal evolution.
For myself I'm not sure there is anything in this. Perhaps the Chinese population is strange, but this seems a very high incidence of a paraprotein in CLL, which we found at only about 2%. I wonder if in China there is a lymphoplasmacytoid lymphoma that closely resembles CLL.
They studied 133 patients with CLL, 86 male and 47 female, median age at diagnosis 60 (range, 44–84). They identified 27 patients with Ig paraproteinemia (12 with IgG, 12 with IgM, 3 with both IgG and IgM, but none with IgA), frequency of 20.3%. The median level of serum IgG paraprotein was 28.2 g/l (range, 21.0–62.0 g/l), and IgM paraprotein was 18.1 g/l (range, 2.3–49.1 g/l). The serum monoclonal Ig light chain concordant with the monoclonal Ig light chain expressed by the neoplastic cells in all patients with Ig paraproteinemia.
Strong correlations of serum Ig paraprotein with advanced Binet stage, DAT-positivity, high level of Beta2-MG and TK1, absence of IGHV mutations, ZAP-70-positivity, CD38-positivity, and cytogenetic abnormalities of del(17p13) or del(11q22)were observed.
With a median follow-up of 36 months (range, 4–83 months), 13 patients (9.8%) died. The prognostic factors with statistical significance were considered in a multivariate Cox regression analysis, del(17p13) ZAP-70, and IgM paraproteinemia were the variables strongly associated with survival.
Ig paraproteinemia was associated with poor outcome. Six (22.2%) with Ig paraproteinemia died during the observation period (2 with IgG paraprotein, 2 with IgM paraprotein, 2 patients with both IgG and IgM, respectively), whereas among the 106 patients without Ig paraproteinemia, 7 (6.6%) died. Patients with Ig paraproteinemia had significantly shorter survival times than patients without serum Ig paraprotein.
Bernstein and colleagues], in a study of 111 patients, reported that the presence of serum monoclonal protein in patients with CLL was associated with a shorter median
survival: 63 months for patients with CLL with serum Ig paraprotein compared with 103 months for patients without serum Ig paraprotein. However, Yin and colleagues have not confirmed this observation. The unfavorable prognostic significance of serum Ig paraprotein was observed in this study.
The possible explanations of discrepancy in prognostic impact of serum Ig paraprotein might be different therapeutic regimens, shorter clinical follow-up and smaller number of patients. retained their capability of isotype switching, a process independent of immunoglobulin heavy chain gene mutation. As an alternative, these additional M components may represent biclonal or triclonal ymphoproliferative disorders as described in the literature or the development of a subclone within the original tumor cells due to clonal evolution.
For myself I'm not sure there is anything in this. Perhaps the Chinese population is strange, but this seems a very high incidence of a paraprotein in CLL, which we found at only about 2%. I wonder if in China there is a lymphoplasmacytoid lymphoma that closely resembles CLL.
Signaling in CLL: opportunities for treatment
Can anything be done at this stage of signaling to block it like Gleevec blocks bcr/abl? Two selective Lyn inhibitors, PP2 and SU6656, block Lyn kinase activity and induce apoptosis, but I know of no trials of these in clinical practice.
Elevated Syk expression by CLL cells results in activation of its downstream targets including Plc2, Erk and Akt. Selective Syk inhibitors BAY-61-3606 and R406 induce apoptosis of CLL cells. siRNA knockdown suggested that constitutively-active Syk maintains high levels of antiapoptotic Mcl-1 via protein kinase C (PKC) δ, which blocks proteasomal degradation of Mcl-1. Downregulation of Mcl-1 in CLL cells treated with Syk inhibitors is consistent with this hypothesis. The susceptibility of CLL cells to apoptosis induction by Syk inhibitors correlated with levels of Syk expression.
In other words Syk signal increase Mcl-1 levels and this seems to be the major agent that stops CLL cells dying. Syk inhibitors might well be effective in treating CLL.
Syk has also been implicated in signalling by chemokines and by integrins. Syk inhibition by R406 or siRNA-mediated knockdown of this PTK abrogated the protective effects of these signals.
Fostamatinib disodium (R788), an orally bioavailable prodrug of R406, blocked BCR signalling in vivo in malignant cells of the Eμ-TCL1 mouse model of CLL, decreased proliferation and survival of malignant cells and prolonged survival of the animals. The drug did not affect the generation of normal B cells. Six of eleven CLL patients treated with fostamatinib showed objective responses in one small clinical trial.
So Fostamatinib shows early promise in treatment. Perhaps in combination with other agents it might be useful.
Imatinib and dasatinib are selective inhibitors of the Abl PTK. Abl expression levels correlated positively with tumour burden and negatively with IGHV mutation levels. Imatinib induced apoptosis of CLL cells that express high levels of Abl. Dasatinib also induced CLL apoptosis in vitro. Dasatinib is a dual inhibitor of Abl and Src PTKs and its critical target with respect to apoptosis induction in CLL cells is not clear at present.
Comment: I think I have already written about Gleevec in CLL.
Elevated Syk expression by CLL cells results in activation of its downstream targets including Plc2, Erk and Akt. Selective Syk inhibitors BAY-61-3606 and R406 induce apoptosis of CLL cells. siRNA knockdown suggested that constitutively-active Syk maintains high levels of antiapoptotic Mcl-1 via protein kinase C (PKC) δ, which blocks proteasomal degradation of Mcl-1. Downregulation of Mcl-1 in CLL cells treated with Syk inhibitors is consistent with this hypothesis. The susceptibility of CLL cells to apoptosis induction by Syk inhibitors correlated with levels of Syk expression.
In other words Syk signal increase Mcl-1 levels and this seems to be the major agent that stops CLL cells dying. Syk inhibitors might well be effective in treating CLL.
Syk has also been implicated in signalling by chemokines and by integrins. Syk inhibition by R406 or siRNA-mediated knockdown of this PTK abrogated the protective effects of these signals.
Fostamatinib disodium (R788), an orally bioavailable prodrug of R406, blocked BCR signalling in vivo in malignant cells of the Eμ-TCL1 mouse model of CLL, decreased proliferation and survival of malignant cells and prolonged survival of the animals. The drug did not affect the generation of normal B cells. Six of eleven CLL patients treated with fostamatinib showed objective responses in one small clinical trial.
So Fostamatinib shows early promise in treatment. Perhaps in combination with other agents it might be useful.
Imatinib and dasatinib are selective inhibitors of the Abl PTK. Abl expression levels correlated positively with tumour burden and negatively with IGHV mutation levels. Imatinib induced apoptosis of CLL cells that express high levels of Abl. Dasatinib also induced CLL apoptosis in vitro. Dasatinib is a dual inhibitor of Abl and Src PTKs and its critical target with respect to apoptosis induction in CLL cells is not clear at present.
Comment: I think I have already written about Gleevec in CLL.
John Trapnell - a sinner saved by grace
I went to the celebration of John Trapnell's life yesterday at Ringwood Parish Church. Although I knew John very well and for a longer period than most of the 300+ in the congregation, there were things I did not know about him. For example, I had not appreciated how much he and I shared similar tastes in music and it would have been great to go to the opera with him. We did have a mutual friend in Peter Witham, who taught my son violin and for many years was my contact with the Bournemouth Symphony Orchestra who often performed for Tenovus, one of the charities that I ran. But John was also involved with the school choir at Ringwood after his retirement, which I knew nothing about.
John had offered in the past to take me sailing, but I was put off by my experience in a sailing dinghy when I was younger. It was a cold and wet endeavour. (Endeavour was the name of Captain James Cook's boat, I believe). John's boats were a little larger than sailing dinghies.
It was good to see some of my old colleagues at the celebration, though fewer than I had hoped. Mostly they were retired and many suffering from the way that old age bites into your life as it does into mine.
Something of John's personality came over. He had insisted to David Craig, his long-time friend and Pastor, that the 'warts' should not be hidden. They were not. John came from a privileged background and led a very blessed life, but there were adversities, some of which were of his own making. He claimed never to have thrown instruments in the Operating Room. He later amended that to saying he had never thrown them at anyone. He was certainly opinionated and some thought him arrogant. But h could be exceedingly humble and he was well aware of his faults. He prayed before every operation and was exceedingly kind to his patients, who genuinely loved him. Some of the things I knew about him are best not said, since they have been repented of and if the Lord can 'see them no more' I don't see why anyone else should.
He was certainly a 'sinner saved by grace' and for those who don't understand that let me explain. Grace is not just a Girl's name, nor something to do with graceful. It has a specific Christian meaning of the unmerited and freely given forgiveness and mercy of God. After I was first converted, my new Pastor, Harry Kilbride, took me for a long walk and taught me the Doctrines of Grace. I have stuck to them ever since.
The Grace doctrines are often described by the acronym TULIP. The T stands for Total depravity. This does not mean that all humans are totally depraved. It sounds really wild in today's world and probably, as words change their meaning, ought to be modified. What it does mean is that every man and woman, every child and baby, has been corrupted by the Fall, and corrupted in every part of their being. It was certainly the case that Adam and Eve were perfect when they were created, but by their wilful disobedience to God, they caused the world and everything in to be cursed. This is known theologically as the Fall. Importantly, it means that every part of Man is corrupted including his will. Of course we are not as bad as we possibly could be. There is still some semblance of what God saw when he pronounced His creation 'good', but it has been marred in every part. Especially this is true about the will. It means that we could not choose to love God with all our heart mind and strength, because our will is corrupt. That choice is not available to us; we will always choose self over God.
That does not prevent us doing good things; atheists may do splendid things, but it stops us from choosing the best. Lutherans tend to believe the same thing on this, but many Methodists were say that their will is free to choose Christ.
The 'U' stands for Unconditional election. This means that God has chosen to save some without regard to whether they were good or bad; without even foreseeing or predestining that they would be come good. It was just an act of love of unmerited mercy. He loved us because he loved us.
There is a danger in this that we should think of ourselves as special, as the chosen people. That is why it must be stressed that this is unmerited. He chose us before the creation of the world because if he had waited to see what we were like he would certainly have discarded us. This is why churches are like hospitals, full of sick people. Never look for perfect Christians in a church; you are sure to be disappointed. An unfortunate correlation with election is that those who are not chosen are condemned. It sounds like God has elected some for damnation - the Lutherans leave this part out completely. But it is open to Man to choose God without His help; it's just that he never does.
The 'L' stands for Limited atonement. Atonement is one of those technical words that mean nothing to most people these days, but it is quite simple. The word means at one ment. It means that we and God are at one with each other. Before, God was angry with the human race because of our disobedience to him. But God had provide the means of assuaging that anger, his son taking the penalty of sin for us on the cross. Many other branches of Christianity believe that the atonememnt was for everybody, but the doctrines of grace suggest it was while potentially sufficient for everybody, in effect it was limited to the elect.
The 'I' stands for Irresistible grace; Lutherans believe it is resistible and Methodists synergistic.
The 'P' stands for the preservation of the saints. It means that once you are saved you cannot be unsaved. Of course some fall away, but they were never saved in the first place - they just gave the appearance of salvation. Lutherans believe that falling away of the saints through apostasy is possible and Methodists that preservation of the saints is conditional on holding on to faith. Some Calvinists are 4 or 4.5 pointers and are less strong on some of these doctrinal points. Among the more famous Calvinists are Jim Packer, Tim Keller and John Piper.
John Trapnell was a five pointer and had good reason to be. Without such grace he could never have been saved.
John had offered in the past to take me sailing, but I was put off by my experience in a sailing dinghy when I was younger. It was a cold and wet endeavour. (Endeavour was the name of Captain James Cook's boat, I believe). John's boats were a little larger than sailing dinghies.
It was good to see some of my old colleagues at the celebration, though fewer than I had hoped. Mostly they were retired and many suffering from the way that old age bites into your life as it does into mine.
Something of John's personality came over. He had insisted to David Craig, his long-time friend and Pastor, that the 'warts' should not be hidden. They were not. John came from a privileged background and led a very blessed life, but there were adversities, some of which were of his own making. He claimed never to have thrown instruments in the Operating Room. He later amended that to saying he had never thrown them at anyone. He was certainly opinionated and some thought him arrogant. But h could be exceedingly humble and he was well aware of his faults. He prayed before every operation and was exceedingly kind to his patients, who genuinely loved him. Some of the things I knew about him are best not said, since they have been repented of and if the Lord can 'see them no more' I don't see why anyone else should.
He was certainly a 'sinner saved by grace' and for those who don't understand that let me explain. Grace is not just a Girl's name, nor something to do with graceful. It has a specific Christian meaning of the unmerited and freely given forgiveness and mercy of God. After I was first converted, my new Pastor, Harry Kilbride, took me for a long walk and taught me the Doctrines of Grace. I have stuck to them ever since.
The Grace doctrines are often described by the acronym TULIP. The T stands for Total depravity. This does not mean that all humans are totally depraved. It sounds really wild in today's world and probably, as words change their meaning, ought to be modified. What it does mean is that every man and woman, every child and baby, has been corrupted by the Fall, and corrupted in every part of their being. It was certainly the case that Adam and Eve were perfect when they were created, but by their wilful disobedience to God, they caused the world and everything in to be cursed. This is known theologically as the Fall. Importantly, it means that every part of Man is corrupted including his will. Of course we are not as bad as we possibly could be. There is still some semblance of what God saw when he pronounced His creation 'good', but it has been marred in every part. Especially this is true about the will. It means that we could not choose to love God with all our heart mind and strength, because our will is corrupt. That choice is not available to us; we will always choose self over God.
That does not prevent us doing good things; atheists may do splendid things, but it stops us from choosing the best. Lutherans tend to believe the same thing on this, but many Methodists were say that their will is free to choose Christ.
The 'U' stands for Unconditional election. This means that God has chosen to save some without regard to whether they were good or bad; without even foreseeing or predestining that they would be come good. It was just an act of love of unmerited mercy. He loved us because he loved us.
There is a danger in this that we should think of ourselves as special, as the chosen people. That is why it must be stressed that this is unmerited. He chose us before the creation of the world because if he had waited to see what we were like he would certainly have discarded us. This is why churches are like hospitals, full of sick people. Never look for perfect Christians in a church; you are sure to be disappointed. An unfortunate correlation with election is that those who are not chosen are condemned. It sounds like God has elected some for damnation - the Lutherans leave this part out completely. But it is open to Man to choose God without His help; it's just that he never does.
The 'L' stands for Limited atonement. Atonement is one of those technical words that mean nothing to most people these days, but it is quite simple. The word means at one ment. It means that we and God are at one with each other. Before, God was angry with the human race because of our disobedience to him. But God had provide the means of assuaging that anger, his son taking the penalty of sin for us on the cross. Many other branches of Christianity believe that the atonememnt was for everybody, but the doctrines of grace suggest it was while potentially sufficient for everybody, in effect it was limited to the elect.
The 'I' stands for Irresistible grace; Lutherans believe it is resistible and Methodists synergistic.
The 'P' stands for the preservation of the saints. It means that once you are saved you cannot be unsaved. Of course some fall away, but they were never saved in the first place - they just gave the appearance of salvation. Lutherans believe that falling away of the saints through apostasy is possible and Methodists that preservation of the saints is conditional on holding on to faith. Some Calvinists are 4 or 4.5 pointers and are less strong on some of these doctrinal points. Among the more famous Calvinists are Jim Packer, Tim Keller and John Piper.
John Trapnell was a five pointer and had good reason to be. Without such grace he could never have been saved.
Stem cell successes
In the past week we have heard of two stem cell successes. In one a man was transplanted with a new trachea (windpipe). A 36-year-old man whose own cancerous trachea had to be removed was treated with the procedure on 9 June at the Karolinska University Hospital in Stockholm, Sweden, by Paolo Macchiarini.
No donor was needed for the new procedure. Instead the tissue was custom-built to fit the patient, then coated inside and out with his own stem cells. The treatment began after Alexander Seifalian of University College London received detailed scans of the patient's diseased trachea. Using these, Seifalian constructed a bespoke replacement from a novel polymeric material that he has developed and patented.
Two days before the operation, the team took 200 ml of bone marrow from the patient and from this extracted 40 ml of mesenchymal stem cells. By pouring these on top of the synthetic organ in a bioreactor developed by Harvard Bioscience of Holliston, Massachusetts, the trachea was successfully coated inside and out with the patient's own cells.
During surgery, Macchiarini's final touch was to add patches of the patient's nose lining to the inner surface of the trachea. These later grew into a layer of epithelial cells matching those lining the inner surfaces of the respiratory tract.
"The big conceptual breakthrough is that we can move from transplanting organs to manufacturing them,” says David Green, the president of Harvard Bioscience – although he adds that the concept would work best for simple structures such as tracheas, ureters and blood vessels.
In another stem cell development, a company called FCB-Pharmicell based in Seongnam, South Korea, became the first in the world to receive official approval for a stem-cell-based procedure to treat people who have survived heart attacks. In the newly approved procedure, stem cells are extracted from the patient's bone marrow, multiplied in the lab then injected directly into the heart through the coronary artery.
Little clinical data is publicly available to prove that the procedure benefits patients, but according to press reports last week, the company says that in trials, patients showed 6 per cent improvements in heart function six months after the procedure, compared with untreated patients.
It is important to recognize that these reports do not derive from embryonic stem cells which have to be produced from spare embryos manufactured by IVF, but from mesenchymal stem cells which come from the patient's own tissue (often bone marrow) that carries neither ethical not rejection risk.
No donor was needed for the new procedure. Instead the tissue was custom-built to fit the patient, then coated inside and out with his own stem cells. The treatment began after Alexander Seifalian of University College London received detailed scans of the patient's diseased trachea. Using these, Seifalian constructed a bespoke replacement from a novel polymeric material that he has developed and patented.
Two days before the operation, the team took 200 ml of bone marrow from the patient and from this extracted 40 ml of mesenchymal stem cells. By pouring these on top of the synthetic organ in a bioreactor developed by Harvard Bioscience of Holliston, Massachusetts, the trachea was successfully coated inside and out with the patient's own cells.
During surgery, Macchiarini's final touch was to add patches of the patient's nose lining to the inner surface of the trachea. These later grew into a layer of epithelial cells matching those lining the inner surfaces of the respiratory tract.
"The big conceptual breakthrough is that we can move from transplanting organs to manufacturing them,” says David Green, the president of Harvard Bioscience – although he adds that the concept would work best for simple structures such as tracheas, ureters and blood vessels.
In another stem cell development, a company called FCB-Pharmicell based in Seongnam, South Korea, became the first in the world to receive official approval for a stem-cell-based procedure to treat people who have survived heart attacks. In the newly approved procedure, stem cells are extracted from the patient's bone marrow, multiplied in the lab then injected directly into the heart through the coronary artery.
Little clinical data is publicly available to prove that the procedure benefits patients, but according to press reports last week, the company says that in trials, patients showed 6 per cent improvements in heart function six months after the procedure, compared with untreated patients.
It is important to recognize that these reports do not derive from embryonic stem cells which have to be produced from spare embryos manufactured by IVF, but from mesenchymal stem cells which come from the patient's own tissue (often bone marrow) that carries neither ethical not rejection risk.
John 5:43. Anyone but Jesus
I have come in my Father’s name, and you do not accept me; but if someone else comes in his own name, you will accept him.
In fact, the Jews followed after several Messianic pretenders. It was a case of anyone but Jesus. They refused to accept anyone preaching the gospel of the suffering servant. Such was their arrogance, they did not see that they were sinners in need of repentance. We are the chosen people. The doctrines of grace are paramount in Christian theology. Followers of Jesus need to recognize their own abject inadequacy and their total dependence on Jesus
In fact, the Jews followed after several Messianic pretenders. It was a case of anyone but Jesus. They refused to accept anyone preaching the gospel of the suffering servant. Such was their arrogance, they did not see that they were sinners in need of repentance. We are the chosen people. The doctrines of grace are paramount in Christian theology. Followers of Jesus need to recognize their own abject inadequacy and their total dependence on Jesus
Tuesday, July 19, 2011
Hizb ut-Tahrir
Our last three Prime Ministers have all wanted to ban the Islamist Group Hizb-ut-Tahrir, but all have failed to do so. Why?
The reason seems to be that current legislation allows the banning of groups that act violently and those that foment violence. Hizb-ut-Tahrir, it seems just have unpleasant views and you can't be banned for those.
This is probably a good thing; otherwise we would be ruled by the thought police. Lord Carlile, the previous counter-terrorism reviewer, said yesterday, "I don't think anything is going to happen … I think the general view is that Hizb ut-Tahrir are best dealt with in public debate rather than by proscription."
They seem to be being defeated in public debate. They had their annual conference in Tower Hamlets recently and the turnout was 200 people, down from several thousand four years ago. This is a group that is rushing towards extinction
The reason seems to be that current legislation allows the banning of groups that act violently and those that foment violence. Hizb-ut-Tahrir, it seems just have unpleasant views and you can't be banned for those.
This is probably a good thing; otherwise we would be ruled by the thought police. Lord Carlile, the previous counter-terrorism reviewer, said yesterday, "I don't think anything is going to happen … I think the general view is that Hizb ut-Tahrir are best dealt with in public debate rather than by proscription."
They seem to be being defeated in public debate. They had their annual conference in Tower Hamlets recently and the turnout was 200 people, down from several thousand four years ago. This is a group that is rushing towards extinction
John 5:41-42. Man-pleasing.
I do not accept praise from men, but I know you do not have the love of God in your hearts.
Most men love the praise of others, but Jesus was only concerned with the praise of God the Father who sent him.
We love to look well in the eyes of other people, but this gets in the way of our love for God and our appreciation of His love for us. What commends us to men? Our wealth? Our cleverness? Our wit? Would that it were our honesty, our humility, or our sacrifice.
Even those who lead us are tempted lest their performance in the pulpit is insufficient or their prayer-life inadequate or their preparation of sermons underdone. It is good to do our best for the Lord, but man-pleasing is not what we are here for.
For those with the love of God in their hearts it is only God they seek to please. Imagine a man besotted with his new wife. Should he treat her in such a way that impresses the neighbors? In no way! His job is to please his new wife.
Most men love the praise of others, but Jesus was only concerned with the praise of God the Father who sent him.
We love to look well in the eyes of other people, but this gets in the way of our love for God and our appreciation of His love for us. What commends us to men? Our wealth? Our cleverness? Our wit? Would that it were our honesty, our humility, or our sacrifice.
Even those who lead us are tempted lest their performance in the pulpit is insufficient or their prayer-life inadequate or their preparation of sermons underdone. It is good to do our best for the Lord, but man-pleasing is not what we are here for.
For those with the love of God in their hearts it is only God they seek to please. Imagine a man besotted with his new wife. Should he treat her in such a way that impresses the neighbors? In no way! His job is to please his new wife.
Signaling in CLL 2
Zap-70 is the PTK that signals in T cells. Although high Zap-70 expression correlates with poor prognosis in CLL, the precise role of this PTK in CLL is not clear.
In Zap-70-positive CLL cells, it becomes tyrosine phosphorylated and associated with CD79b following BCR engagement and indeed tyrosine phosphorylation of Syk is greater than in Zap-70-negative cells. If you transduce Zap-70 into CLL cells there is enhanced BCR signalling, but this is independent of the PTK activity of Zap-70. Zap-70 may therefore function either as an adaptor protein that augments Syk activation or as a decoy that sequesters a negative regulator of Syk.
Zap-70 may contribute to drug resistance by enhancing migratory responses of CLL cells to the chemokines CCL 19 and 21, thus promoting migration of malignant cells to sites where apoptosis resistance is enhanced by microenvironmental signalling.
The RhoH guanine nucleotide-binding protein contains ITAM motifs and is an adaptor that recruits Zap-70 to T lymphocyte antigen receptors. RhoH is overexpressed in CLL cells relative to normal B cells. Deletion of RhoH retards progression of the CLL-like disease of Eμ-TCL-1 transgenic mice, implying that overexpression of RhoH contributes to CLL pathology by augmenting the contribution of Zap-70 to antigen receptor signalling.
In lay language: Although ZAP-70 positive CLL cells are more malignant, ZAP-70 does not take part in the active signaling process in CLL, the way it does in T-cells. It may act either as an enhancer of Syk activation or as a suprressor of Syk inhibition. It also may act by increasing the response of CLL cells to chemokines, so pushing them into parts of the microenvironment where there are other factors producing resistance to apoptosis.
RhoH is another signaling protein that is important in T cells that is increased in CLL cells. In the TCL-1 animal model for CLL, the disease is retarded if RhoH is deleted, which implies it might have an active role in CLL like that of Zap-70.
In Zap-70-positive CLL cells, it becomes tyrosine phosphorylated and associated with CD79b following BCR engagement and indeed tyrosine phosphorylation of Syk is greater than in Zap-70-negative cells. If you transduce Zap-70 into CLL cells there is enhanced BCR signalling, but this is independent of the PTK activity of Zap-70. Zap-70 may therefore function either as an adaptor protein that augments Syk activation or as a decoy that sequesters a negative regulator of Syk.
Zap-70 may contribute to drug resistance by enhancing migratory responses of CLL cells to the chemokines CCL 19 and 21, thus promoting migration of malignant cells to sites where apoptosis resistance is enhanced by microenvironmental signalling.
The RhoH guanine nucleotide-binding protein contains ITAM motifs and is an adaptor that recruits Zap-70 to T lymphocyte antigen receptors. RhoH is overexpressed in CLL cells relative to normal B cells. Deletion of RhoH retards progression of the CLL-like disease of Eμ-TCL-1 transgenic mice, implying that overexpression of RhoH contributes to CLL pathology by augmenting the contribution of Zap-70 to antigen receptor signalling.
In lay language: Although ZAP-70 positive CLL cells are more malignant, ZAP-70 does not take part in the active signaling process in CLL, the way it does in T-cells. It may act either as an enhancer of Syk activation or as a suprressor of Syk inhibition. It also may act by increasing the response of CLL cells to chemokines, so pushing them into parts of the microenvironment where there are other factors producing resistance to apoptosis.
RhoH is another signaling protein that is important in T cells that is increased in CLL cells. In the TCL-1 animal model for CLL, the disease is retarded if RhoH is deleted, which implies it might have an active role in CLL like that of Zap-70.
Monday, July 18, 2011
Understanding cell signaling

My old friend Stan Wickremasinghe has written a beautiful review of signalling in Brit J Haem and I intend to use it as a teaching tool on this blog. This will be a series of blogs because my experience is that I can only really take in about one fact at a time and since this isn't really my field, I shall be learning too.
The B-cell receptor (BCR) is the B-cells gateway to the outside world. It is in fact an antibody molecule, designed to recognize the antigen that the B-cell is programmed to react with. But it does not connect to anything inside the cell. For this it has to interact with the Ig associated molecules CD79a and CD79b.
When the BCR transmembrane immunoglobulin molecule is engaged by antigen the CD79 a and b proteins of the BCR, the Protein Tyrosine Kinase (PTK), Lyn, is activated. Phosphorylation of tyrosine residues within an immune receptor tyrosine-based activation motif (ITAM) sequence in the C-terminal tail of the CD79 molecules results in recruitment of an additional PTK, Syk, resulting in generation of further phosphotyrosine sites. Binding of the SH2-containing protein phosphatase 1 (Shp1) to immune receptor tyrosine-based inhibitor motifs (ITIMs) on transmembrane molecules (including CD22) results in dephosphorylation of phosphotyrosines, providing negative regulation of BCR signalling.
In plain English, in a B-cell, the immunoglobulin molecule on the surface binds to the antigen it was designed for - eg an anti-measles antibody binds to a measles virus. But a CLL cell is probably only rarely designed to fight measles - it looks like the target for CLL cells are proteins released from dying cells in many cases. The immunoglobulin molecule needs an auxiliary molecule to help it signal - this is CD79 (often low in CLL, so is this why it often does not signal very well?)
Activation of CD79 alerts two tyrosine kinases, Lyn and Syk, which are capable of sending messages onward through the cell. Lyn, at least, is thought to act like a rheostat, controling the strength of signal that is sent onwards. It seems to do this by invoking a suppressing signal, binding to the inhibitory protein Shp1 on CD22, which is normally present on B-cells in association with the BCR. (But surface CD22 on CLL cells is either absent or very reduced. It can be detected intracellularly though. Is there more to learn here?)
Family matters
The newspapers are full of the phone hacking fiasco and the public is bored by it. Newspapers think that their little world is important but nobody else does.
Let's talk about cricket instead. My son's team played in the 20/20 final of the South Northamptonshire cricket league. In a low scoring match on a rain affected pitch his team was all out for 82 of which he scored 22. Then the opposition were bowled out for 61 of which he took 4-17 in 4.2 overs. He got man-of-match, cut the grass and made the tea.
His team are top of division 5 and with only 5 more games before the end of the season look like being promoted.
He is off in Italy at the present preparing for the NASCAR series. It's a nice life if you don't weaken.
Today Karen returns from her holiday in Jamaica and Angela starts hers in the Lake District. Contrasting weather! Angela has taken her lap-top so I imagine that she will be writing up her PhD is the weather sets in.
Richard will be in the Isle of Wight when the school holidays begin.
We had a new front lawn laid over the weekend and today. Good weather for lawn laying - cool and wet.
Health has not been special these last few days. I'm very tired after meals and bloating has got worse.
Let's talk about cricket instead. My son's team played in the 20/20 final of the South Northamptonshire cricket league. In a low scoring match on a rain affected pitch his team was all out for 82 of which he scored 22. Then the opposition were bowled out for 61 of which he took 4-17 in 4.2 overs. He got man-of-match, cut the grass and made the tea.
His team are top of division 5 and with only 5 more games before the end of the season look like being promoted.
He is off in Italy at the present preparing for the NASCAR series. It's a nice life if you don't weaken.
Today Karen returns from her holiday in Jamaica and Angela starts hers in the Lake District. Contrasting weather! Angela has taken her lap-top so I imagine that she will be writing up her PhD is the weather sets in.
Richard will be in the Isle of Wight when the school holidays begin.
We had a new front lawn laid over the weekend and today. Good weather for lawn laying - cool and wet.
Health has not been special these last few days. I'm very tired after meals and bloating has got worse.
John 5:39-40. Blind to Scripture
You diligently study the Scriptures because you think by them you possess eternal life. These are the Scriptures that testify about me yet you refuse to come to me to have life.
As evangelicals we set great store by the Scripture. We believe that every word is 'God-breathed'. We admit to no changes to what was originally given. We believe them to be historically true, even when the whole of modern science is set against some of them.
The Pharisees too set great store by the Scripture. When the Scribes were copying them they assigned a number to each letter and added up each row and column as a guard against error creeping in. But of more importance than the book is what it says. When Jesus opened up the Scriptures on the road to Emmaus is was clear that even his disciples didn't understand what the Old Testament was saying about him.
The Pharisees were more fortunate than we; they didn't just have the Scripture; they had Jesus. You see you need the Holy Spirit's eyes to read the Word of God.
As evangelicals we set great store by the Scripture. We believe that every word is 'God-breathed'. We admit to no changes to what was originally given. We believe them to be historically true, even when the whole of modern science is set against some of them.
The Pharisees too set great store by the Scripture. When the Scribes were copying them they assigned a number to each letter and added up each row and column as a guard against error creeping in. But of more importance than the book is what it says. When Jesus opened up the Scriptures on the road to Emmaus is was clear that even his disciples didn't understand what the Old Testament was saying about him.
The Pharisees were more fortunate than we; they didn't just have the Scripture; they had Jesus. You see you need the Holy Spirit's eyes to read the Word of God.